Downloaded 103 times

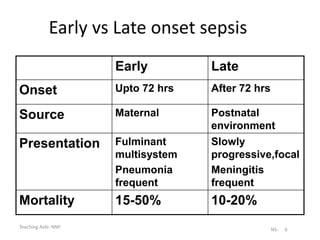
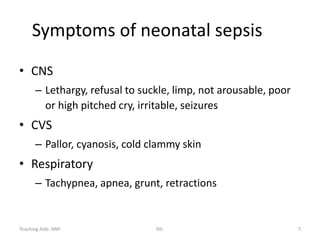
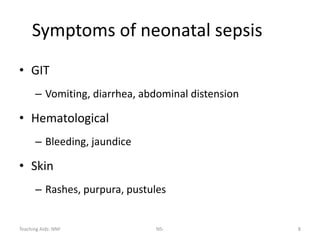

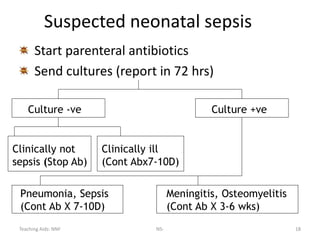
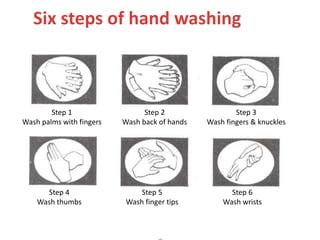

Neonatal sepsis is a major cause of neonatal mortality in developing countries, contributing to about 30-50% of deaths. The incidence of neonatal sepsis in India is approximately 30 per 1000 live births. Sepsis can be either early-onset (within 72 hours of birth) or late-onset, and is usually caused by organisms like Klebsiella pneumoniae, E. coli, and Staphylococcus aureus. Diagnosis involves clinical signs and symptoms as well as screening tests and blood/CSF cultures. Treatment consists of supportive care and parenteral antibiotics like ampicillin and aminoglycosides. Prevention emphasizes handwashing, hygiene, and infection control practices.































![Sepsis neonatal [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/sepsisneonatalautoguardado-170318103240-thumbnail.jpg?width=640&height=640&fit=bounds)

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

