Downloaded 311 times







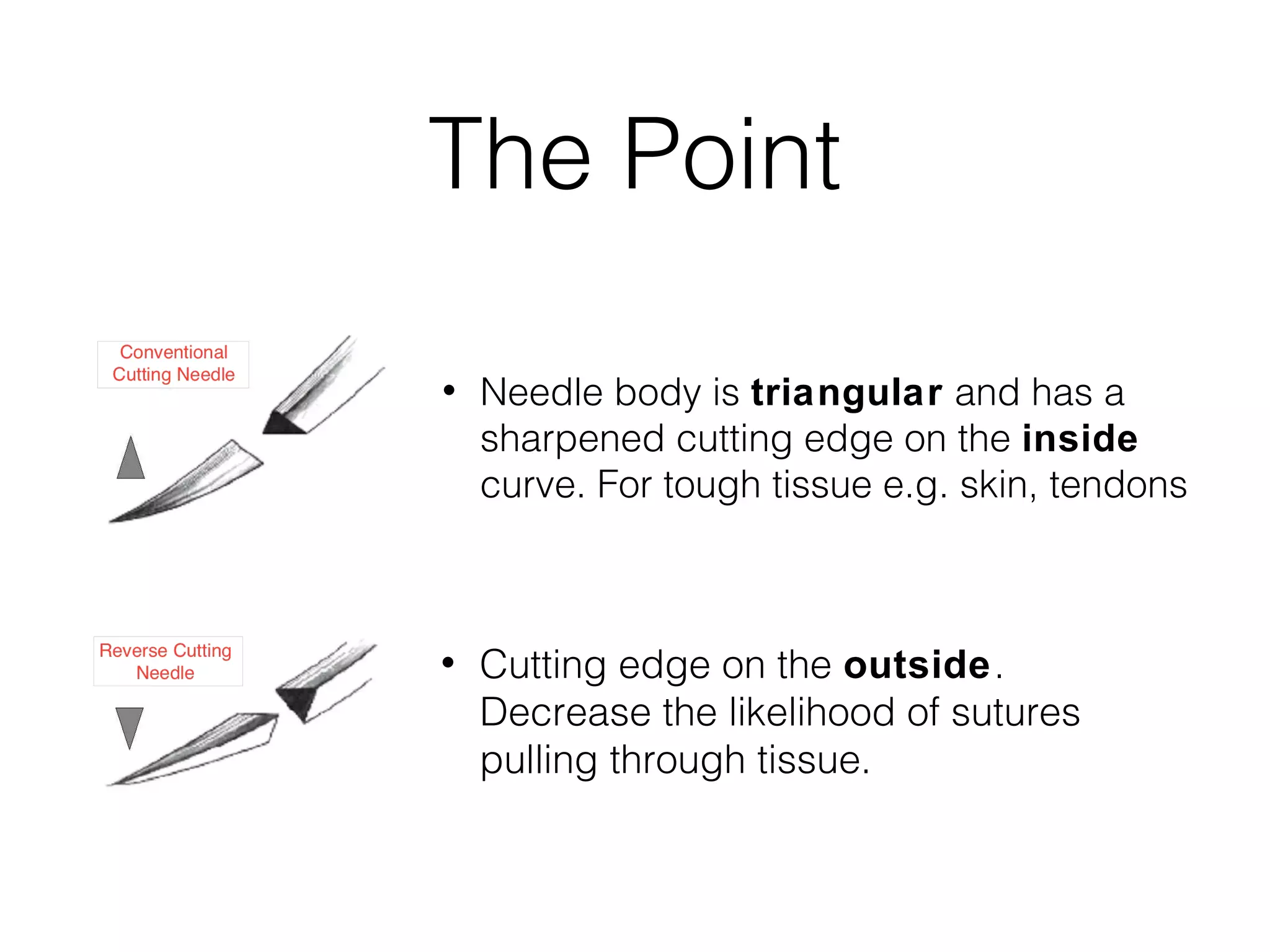





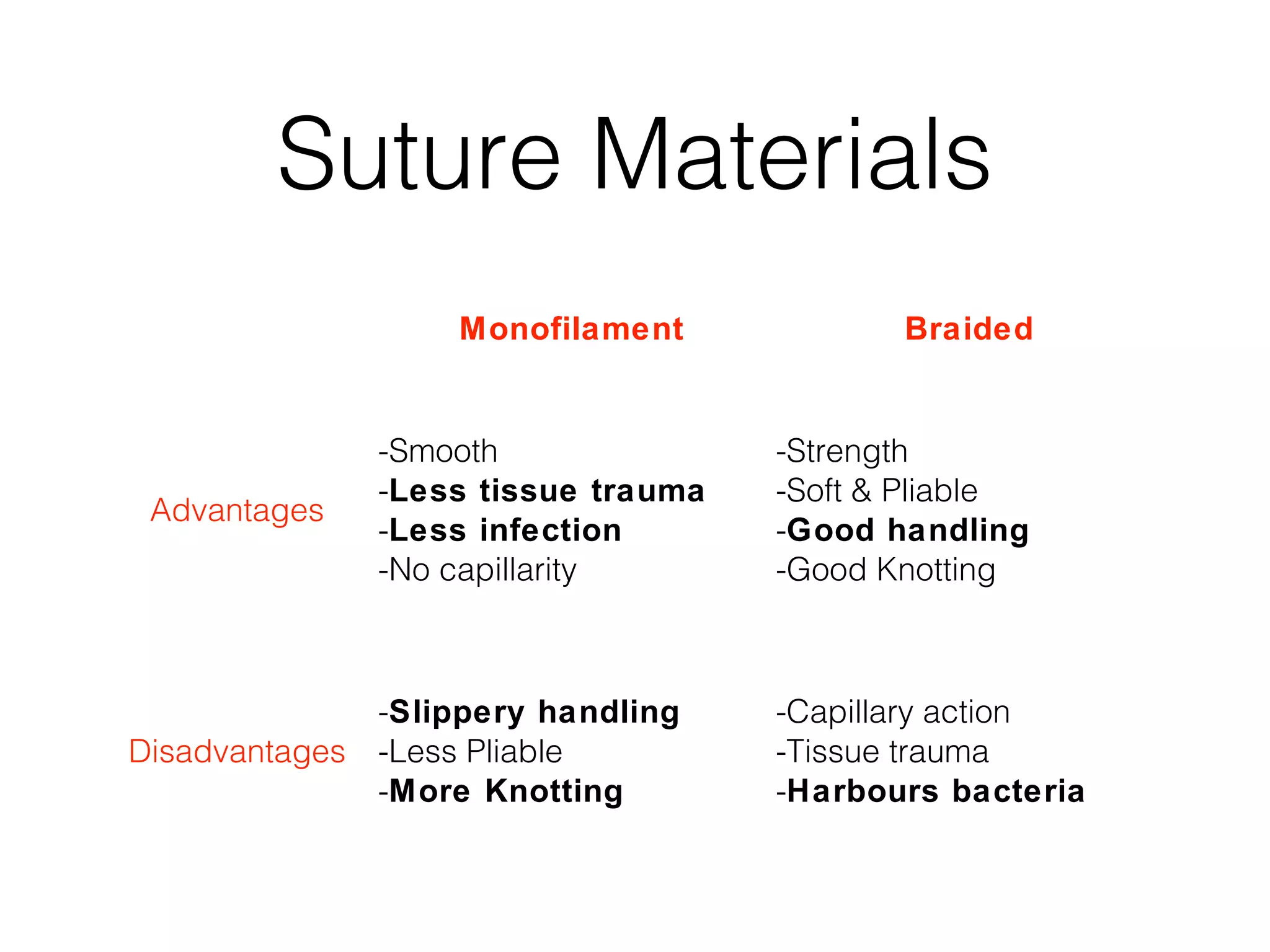







This document provides a summary of the history and types of needles and sutures used in surgery. It discusses key historical landmarks in suture development, including the earliest known medical records describing sutures from Ancient Egypt. It also outlines the development of mass-produced sterile catgut sutures in the late 19th century. The document describes the anatomy of surgical needles and various suture materials, sizes, and packaging. It compares absorbable and non-absorbable, natural and synthetic, monofilament and braided suture types. Finally, it discusses ideal suture characteristics and factors to consider when selecting a suture for a procedure.





















































































