Downloaded 844 times
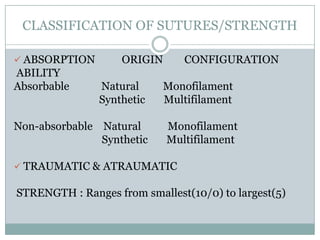
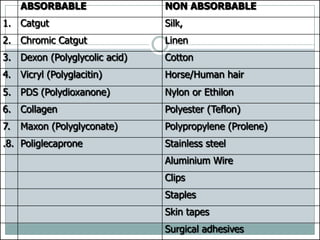
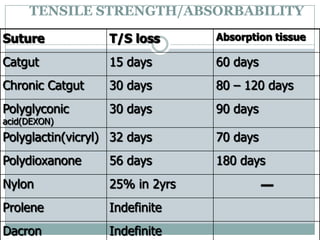


The document discusses sutures and suturing techniques in surgery, outlining their historical background, definitions, types, properties, and uses. It covers various suture materials, their classifications, and suitability for different surgical procedures, along with advances in suturing methods such as staples and adhesives. The importance of selecting appropriate sutures for optimal healing and minimal complications is emphasized.















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





