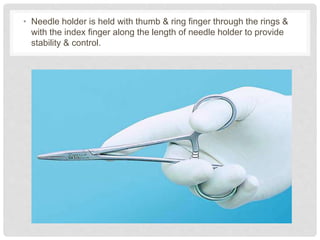
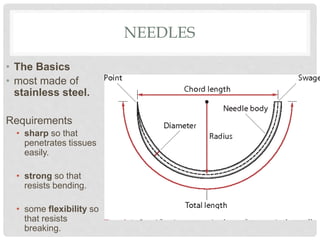
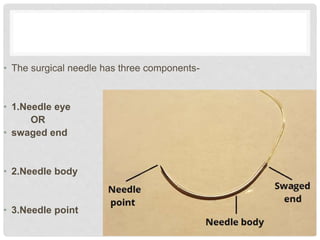
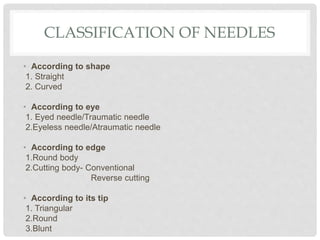
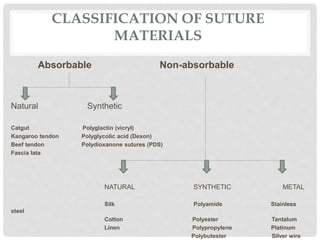
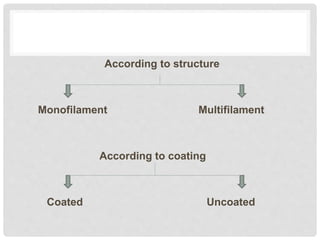
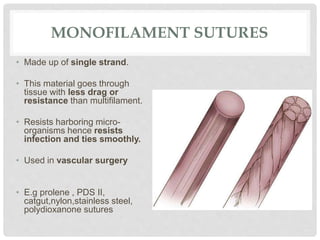
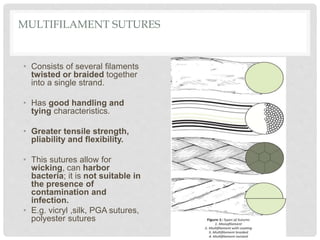
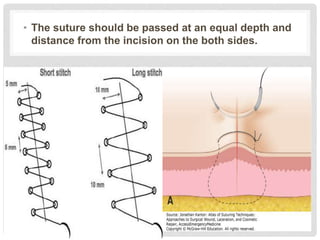
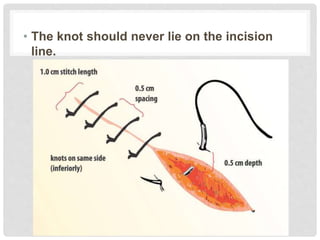
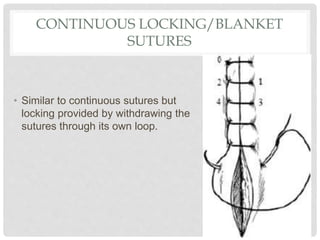
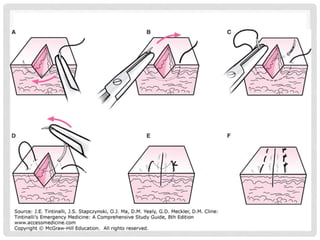
This document provides information on suture materials and techniques. It discusses the anatomy of skin, definitions of suturing terms, goals of suturing, ideal suture requirements, suturing armamentarium including needles and needle holders. It also covers various suture materials like catgut, silk, nylon, linen; their properties, manufacturing process, sterilization methods and uses. Principles of suture selection and different suturing techniques are also explained.