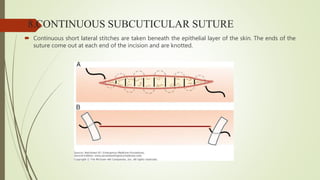
Suturing is performed to approximate tissue and hold wounds closed until healing occurs. There are various suture materials that can be used including natural, synthetic, and metallic options. Key factors in choosing a suture include tensile strength, biocompatibility, absorption rate, and handling properties. Common techniques for placing sutures include simple interrupted, continuous, mattress stitches, and subcuticular sutures. Proper knot tying is also important to secure tissues without causing damage or tension.