Suturing
Suturing of thesurgical wound is necessary, aiming at:
❑Holding a flap over the wound.
❑Reapproximating the wound edges.
❑Protecting underlying tissues from infection or other irritating
factors.
❑Minimal scarring, maximal esthetic results.
❑Earlier return to function.
❑Speeds healing process.
❑Reduces pain.
❑Preventing postoperative hemorrhage.
3.
Suturing may alsoaid in the following:
❑For laceration of soft tissues in general.
❑When hemorrhage is present deep in the tissues and
ligation is required.
❑ In cases of severe hemorrhage where the suture
holds the haemostatic plug in place.
❑ For infections, after stap incision, for stabilization of
the rubber drain at the site of incision.
❑ For immobilization of pedicle flaps in their new
position.
❑For traction of flaps and tissues.
6.
Suturing needle
Ideal surgicalneedle characteristics:
❑High-quality stainless steel.
❑Sterile and corrosion-resistant to prevent introduction of
microorganisms or foreign materials into the wound.
❑Suitable diameter as possible.
❑Stable in the grasp of the needle holder.
❑Capable of implanting suture material through tissue with minimal
trauma.
❑Sharp enough to penetrate tissue with minimal resistance.
7.
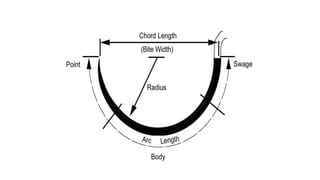
The Needle:
Every surgicalneedle has three basic components: eye; body; and point.
The eye of the needle: may be eyed, or eyeless (swaged).
The body of the needle: is the portion, which is grasped by the needle holder
during the surgical procedure. The body of the needle should be as close as
possible to the diameter of the suture material to minimize bleeding and leakage.
By its body, the needle may be straight, or curved.
The point of the needle: extends from the extreme tip of the needle to the
maximum cross-section of the body. By its point, the needle may be tapered or
cutting.
10.
Types of theneedles
According to the eye:
I- The closed eye (eyed) needle:
1. It is similar to a household sewing needle. The shape of the eye may
be round, oblong, or square.
2. It must be threaded. This in turn presents some disadvantages:
• Procedure is time-consuming.
• It necessitates tying the suture to the eye to minimize unthreading
during use, a case that adds to the bulk of the suture.
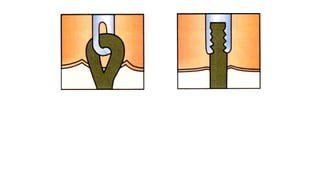
• It entails pulling a double strand of suture material through tissue,
creating a larger hole with additional tissue disruption.
3. It can be sterilized and reused. However, repeated use causes the
needle to become dull, thereby making suturing more difficult.
12.
II- Eyeless needle:
1.Most needles used today are swaged.
2. Handling and preparation are minimized.
3. Tissues are subjected to minimal trauma.
4. Inventory and time spent cleaning, sharpening,
handling, and sterilizing reusable eyed-needles is
eliminated, thereby reducing cost as well as risk of
needle punctures.
5.Swaged sutures eliminate suture damage due to sharp
comers in the eye of eyed needles.
16.
Advantages of EyelessNeedles
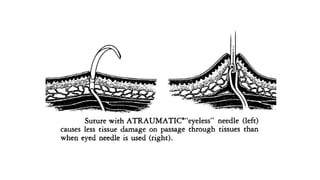
•Less trauma to the tissues, since a single strand of suture material
has to be drawn through the tissues and this creates a smaller hole.
•Each patient has the benefit of a new, sharp, guaranteed sterile
needle.
•Decrease chances of accidental unthreading of the needle and
losing it while suturing.
•Faster and more efficient procedure.
•Needles are made up of high quality steel.
•Time saving: no need of cleaning, sterilizing and threading the eyed
needles.
17.
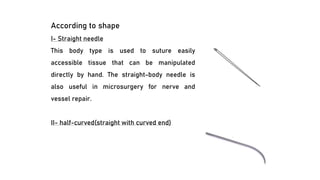
According to shape
I-Straight needle
This body type is used to suture easily
accessible tissue that can be manipulated
directly by hand. The straight-body needle is
also useful in microsurgery for nerve and
vessel repair.
II- half-curved(straight with curved end)
18.
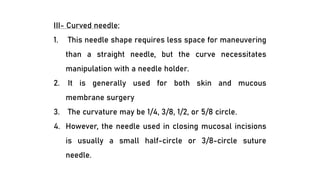
III- Curved needle:
1.This needle shape requires less space for maneuvering
than a straight needle, but the curve necessitates
manipulation with a needle holder.
2. It is generally used for both skin and mucous
membrane surgery
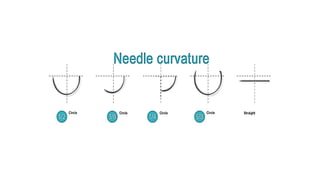
3. The curvature may be 1/4, 3/8, 1/2, or 5/8 circle.
4. However, the needle used in closing mucosal incisions
is usually a small half-circle or 3/8-circle suture
needle.
20.
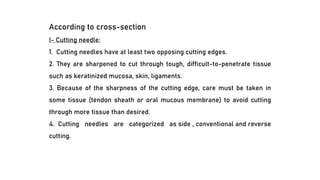
According to cross-section
I-Cutting needle:
1. Cutting needles have at least two opposing cutting edges.
2. They are sharpened to cut through tough, difficult-to-penetrate tissue
such as keratinized mucosa, skin, ligaments.
3. Because of the sharpness of the cutting edge, care must be taken in
some tissue (tendon sheath or oral mucous membrane) to avoid cutting
through more tissue than desired.
4. Cutting needles are categorized as side , conventional and reverse
cutting.
21.
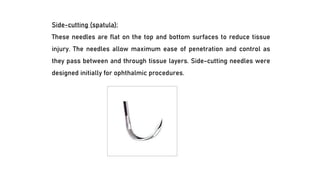
Side-cutting (spatula):
These needlesare flat on the top and bottom surfaces to reduce tissue
injury. The needles allow maximum ease of penetration and control as
they pass between and through tissue layers. Side-cutting needles were
designed initially for ophthalmic procedures.
22.
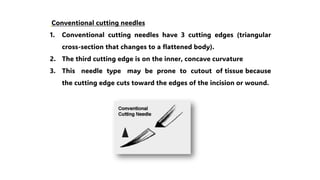
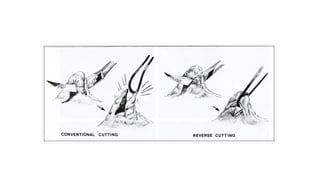
Conventional cutting needles
1.Conventional cutting needles have 3 cutting edges (triangular
cross-section that changes to a flattened body).
2. The third cutting edge is on the inner, concave curvature
3. This needle type may be prone to cutout of tissue because
the cutting edge cuts toward the edges of the incision or wound.
23.
Reverse cutting needles:
1.The reverse cutting needle is as sharp as the conventional cutting needle, but
its design is distinctively different.
2. The third cutting edge is located on the outer convex curvature of the needle.
This offers some advantages:
• Reverse cutting needles have more strength than similar-sized conventional
cutting needles.
•The danger of tissue cutout is greatly reduced.
• The hole left by the needle leaves a wide wall of tissue against which the
suture is to be tied.
25.
II- Taper Point(round) Needle:
1. Also referred to as round needles, taper point needles pierce and
spread tissue without cutting it.
2. The needle point tapers to a sharp tip. The needle body then flattens to
an oval or rectangular shape. This increases the width of the body to
help prevent twisting or turning in the needle holder.
3. Taper point needles are usually used in easily penetrated tissue such
as viscera, oral mucosa, and subcutaneous layers.
4. They are preferred when the smallest possible hole in the tissue and
minimum tissue cutting are desired.
Ideal suture characteristics
Theideal suture has the following characteristics:
•Sterile
•Causes minimal tissue injury or tissue reaction.
•Easy to handle (pliability)
•Holds securely when knotted (high knot strength).
•High tensile strength
•Uniform diameter and size
•Favorable absorption profile
•Resistant to infection
Unfortunately, at present, no single material can provide all of these
characteristics.
28.
Suture size
Size refersto the diameter of the suture strand and is denoted as
zeroes. The more zeroes characterizing a suture size, the smaller the
resultant strand diameter (e.g. 4-0 or 0000 is larger than 5-0 or 00000).
The smaller the suture, the less tensile strength of the strand. 3-0 and
4-0 sutures are the most common used in oral surgery.
30.
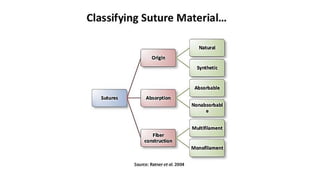
Monofilament versus multifilamentsutures
Monofilament suture
❑is made of a single strand.
❑This structure is relatively more resistant to harboring microorganisms.
❑The monofilament sutures exhibit less resistance to passage through tissue
than multifilament suture.
❑Great care must be taken in handling and tying monofilament suture because
crushing or crimping of this suture can nick or weaken the suture and lead to
undesirable and premature suture failure.
31.
Multifilament suture:
❑It iscomposed of several filaments twisted or braided together.
❑These materials are less stiff but have a higher coefficient of
friction when the suture is passed through tissue. Multifilament
sutures are often treated with special coatings to allow tissue
passage to occur more easily and to reduce subsequent tissue
damage.
❑ Multifilament suture generally has greater tensile strength and
better pliability and flexibility than monofilament suture.
❑This type of suture handles and ties well.
❑Because multifilament materials have increased capillarity, the
increased absorption of fluid may act as a tract for the introduction
of pathogens.
32.
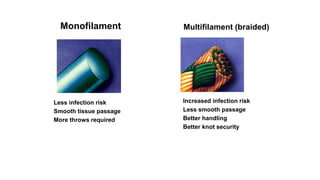
Less infection risk
Smoothtissue passage
More throws required
Monofilament
Increased infection risk
Less smooth passage
Better handling
Better knot security
Multifilament (braided)
33.
Absorbable versus nonabsorbablesutures
Absorbable sutures provide temporary wound support, until the wound heals well
enough to withstand normal stress. Absorption occurs by enzymatic degradation in
natural materials and by hydrolysis in synthetic materials. Hydrolysis causes less
tissue reaction than enzymatic degradation.
Accelerated absorption may occur in patients with fever, infection, or protein
deficiency and may lead to an excessively rapid decline in tensile strength.
Accelerated absorption may also occur in a body cavity that is moist or filled with
fluid or if sutures become wet or moist during handling prior to implantation.
Nonabsorbable sutures elicit a tissue reaction that results in encapsulation of the
suture material by fibroblasts. Including silk, cotton, polyesters, linen, prolene,
stainless steel, etc…….
34.
Natural or synthetic:
-Suturescan be made from natural materials: for example, catgut, silk, or
cotton, and several synthetic absorbable and nonabsorbable sutures are
also available.
•Natural sutures tend to cause an inflammatory tissue reaction.
•Synthetic absorbable sutures are made from long chains of polymers
braided into suture material. Examples are polyglycolic acid and polylactic
acid.
•Synthetic nonabsorbable sutures are made from fibers of polyester,
polypropylene, or polyethylene.
35.
Absorbable Sutures
The absorbablesurgical sutures are made from either "natural "or synthetic
polymers.
Natural
1. Cat gut
2. Plain surgical gut
3. Chromic surgical gut
Synthetic
1. Polyglycolic acid(Dexon)
2. Vicryl (polyglactin):
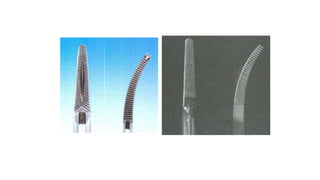
The Needle Holder
❑The needle holder is used to pass a suture needle through tissue.
❑ It must be made of non-corrosive, high strength, good quality steel
alloy with beaks designed for holding the surgical needle securely.
❑ The beak of the needle holder is shorter and stronger than the beak of
the hemostat.
❑ The beak of the needle holder has a crosshatched face to allow positive
grasp of the suture needle, while the face of the beak hemostat has
parallel grooves, which decrease the control over the suture needle.
❑ Most, but not all, needle holders have a ratchet lock near to thumb and
finger rings.
43.
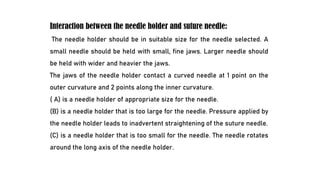
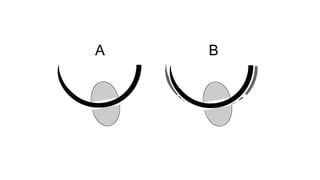
Interaction between theneedle holder and suture needle:
The needle holder should be in suitable size for the needle selected. A
small needle should be held with small, fine jaws. Larger needle should
be held with wider and heavier the jaws.
The jaws of the needle holder contact a curved needle at 1 point on the
outer curvature and 2 points along the inner curvature.
( A) is a needle holder of appropriate size for the needle.
(B) is a needle holder that is too large for the needle. Pressure applied by
the needle holder leads to inadvertent straightening of the suture needle.
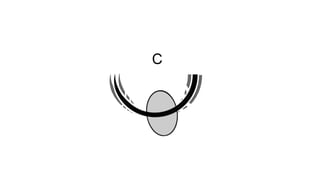
(C) is a needle holder that is too small for the needle. The needle rotates
around the long axis of the needle holder.
46.
The needle holdercan be used:
❑ to pass a suture needle through tissue.
❑ Loading surgical blade to the handle and removal the blade from
handle.
❑ Wiring in fixation of fractures.
48.
Scissors
Suture scissors:
have relativelylong handles and thumb and finger rings. They are held
in the same way as the needle holder, and usually have short cutting
edges, because their sole purpose is to cut sutures.
Tissue scissors:
used for undermining soft tissue, and cutting tissues.
Tissue scissors should not be used to cut sutures, because the suture
material will dull the edges of the blades and make them less
effective for cutting tissue.
51.
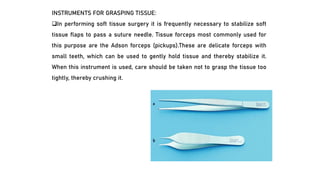
INSTRUMENTS FOR GRASPINGTISSUE:
❑In performing soft tissue surgery it is frequently necessary to stabilize soft
tissue flaps to pass a suture needle. Tissue forceps most commonly used for
this purpose are the Adson forceps (pickups).These are delicate forceps with
small teeth, which can be used to gently hold tissue and thereby stabilize it.
When this instrument is used, care should be taken not to grasp the tissue too
tightly, thereby crushing it.
52.
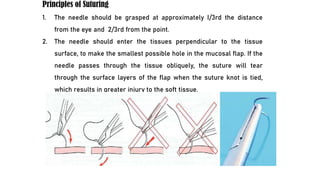
Principles of Suturing
1.The needle should be grasped at approximately I/3rd the distance
from the eye and 2/3rd from the point.
2. The needle should enter the tissues perpendicular to the tissue
surface, to make the smallest possible hole in the mucosal flap. If the
needle passes through the tissue obliquely, the suture will tear
through the surface layers of the flap when the suture knot is tied,
which results in greater injury to the soft tissue.
53.
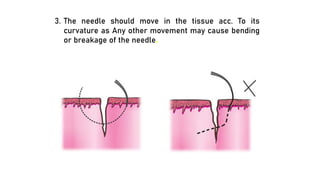
3. The needleshould move in the tissue acc. To its
curvature as Any other movement may cause bending
or breakage of the needle.
54.
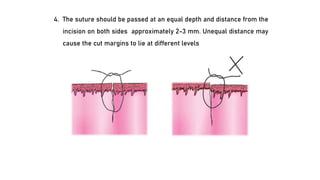
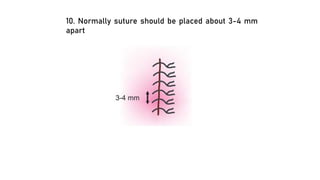
4. The sutureshould be passed at an equal depth and distance from the
incision on both sides approximately 2-3 mm. Unequal distance may
cause the cut margins to lie at different levels
55.
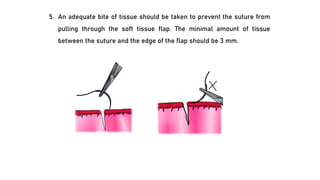
5. An adequatebite of tissue should be taken to prevent the suture from
pulling through the soft tissue flap. The minimal amount of tissue
between the suture and the edge of the flap should be 3 mm.
56.
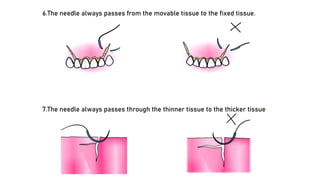
6.The needle alwayspasses from the movable tissue to the fixed tissue.
7.The needle always passes through the thinner tissue to the thicker tissue.
57.
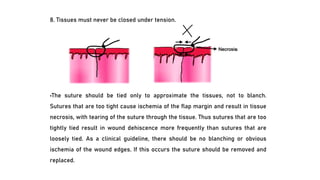
8. Tissues mustnever be closed under tension.
•The suture should be tied only to approximate the tissues, not to blanch.
Sutures that are too tight cause ischemia of the flap margin and result in tissue
necrosis, with tearing of the suture through the tissue. Thus sutures that are too
tightly tied result in wound dehiscence more frequently than sutures that are
loosely tied. As a clinical guideline, there should be no blanching or obvious
ischemia of the wound edges. If this occurs the suture should be removed and
replaced.
58.
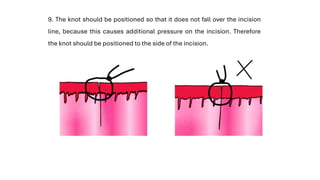
9. The knotshould be positioned so that it does not fall over the incision
line, because this causes additional pressure on the incision. Therefore
the knot should be positioned to the side of the incision.
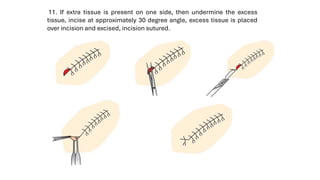
11. If extratissue is present on one side, then undermine the excess
tissue, incise at approximately 30 degree angle, excess tissue is placed
over incision and excised, incision sutured.
61.
•If a threecornered flap is used, the vertical end of the incision must be closed
separately. Two sutures usually are required to close the vertical end properly.
Before the sutures are inserted, the Woodson periosteal elevator should be
used to elevate slightly the non-flap side of the incision, freeing the margin to
facilitate passage of the needle through the tissue. The first suture is placed
across the papilla, where the vertical release incision was made. This is a
known, easily identifiable land-mark that is most important when repositioning
a three cornered flap. The remainder of the envelope portion of the incision is
then closed, after which the vertical component is closed. The slight reflection
of the non-flap side of the incision greatly eases the placing of sutures.
•The sutures are left in place for approximately 5 to 7 days. After this time they
play no useful role and, in fact, probably increase the contamination of the
underlying submucosa.
Interrupted(simple) Suture:
This isthe simplest and most frequently used type, and may be used in
all surgical procedures of the mouth. The needle enters 3 mm away
from the margin of the flap (mobile tissue) and exits at the same
distance on the opposite side. The two ends of the suture are then tied
in a knot and are cut 5 mm above the knot. To avoid tearing the flap, the
needle must pass through the wound margins one at a time, and be at
least 3 mm away from the edges. Over-tightening of the suture must
also be avoided (risk of tissue necrosis), as well as overlapping of
wound edges when positioning the knot. The advantage of the
interrupted suture is that when sutures are placed in a row,
inadvertent loosening of one or even losing one will not influence the
rest.
67.
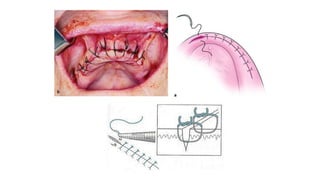
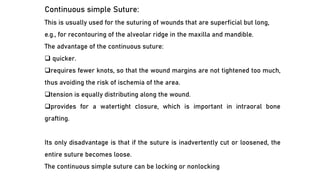
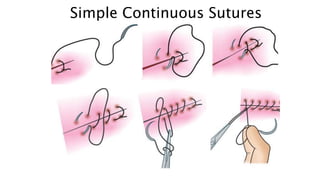
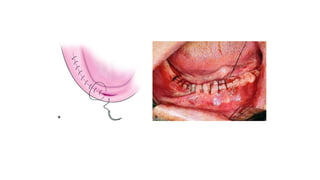
Continuous simple Suture:
Thisis usually used for the suturing of wounds that are superficial but long,
e.g., for recontouring of the alveolar ridge in the maxilla and mandible.
The advantage of the continuous suture:
❑ quicker.
❑requires fewer knots, so that the wound margins are not tightened too much,
thus avoiding the risk of ischemia of the area.
❑tension is equally distributing along the wound.
❑provides for a watertight closure, which is important in intraoral bone
grafting.
Its only disadvantage is that if the suture is inadvertently cut or loosened, the
entire suture becomes loose.
The continuous simple suture can be locking or nonlocking
68.
Non- locking continuoussuture:
The technique applied is as follows:
❑After passing the needle through both flap margins, an initial knot is made
just as in the interrupted suture but only the free end of the suture is cut off.
❑The needle-bearing suture is then used to create successive continuous
sutures at the wound margins.
❑The last suture is not tightened, but the loop created actually serves as the
free end of the suture. Afterwards, the needle bearing suture is wrapped
around the needle holder twice, which grasps the curved suture (first loop),
pulling it through the second loop. The two ends are tightened, thus creating
the surgeon’s knot.
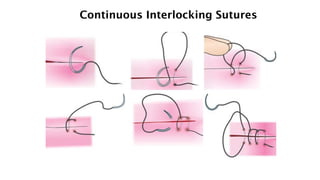
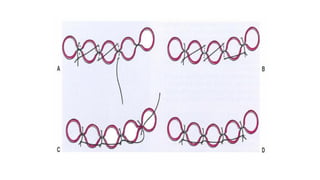
The continuous locking(looping)suture:
❑This type of suture is created exactly as non-locking continuous
suture, except that the needle passes through every loop before
passing through the tissues, which secures the suture after tightening.
Suturing continues with the creation of such loops, which make up
parts of a chain along the incision These loops are positioned on the
buccal side of the wound, after being tightened.
❑This technique more accurately approximates tissue margins than
does the continuous simple technique.
❑It aligns itself perpendicular to the incision, and the locking feature
prevents continuous tightening of the suture as wound closure
progresses
❑this suture is less prone to become loose if the ends should become
untied
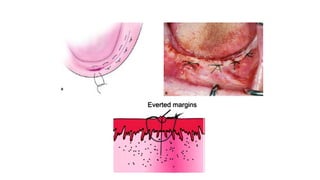
Mattress Sutures:
This isa special type of suture and is described as horizontal
(interrupted and continuous) and vertical. It is indicated in cases:
❑ where strong and secure re-approximation of wound margins is
required, and to resist muscle pull (this will reduce the risk of wound
dehiscence).
❑ to evert the wound edges (which keeps epithelium away from
underlying structures.
❑ to adapt the tissue flaps tightly to underlying structures when a bone
graft or regenerative membrane is used, or during dental implant
surgery.
78.
The vertical suturemay be used for deep incisions, while the horizontal suture
is used in cases which require limiting or closure of soft tissues over osseous
cavities, e.g., postextraction tooth sockets.
The technique used for the mattress suture is as follows:
in the interrupted suture (horizontal and vertical), the needle passes through
the wound margins at a right angle, and the needle always enters and exits the
tissues on the same side.
In the horizontal continuous suture, after creating the initial knot, the needle
enters and exits the tissues in a winding maze pattern. The final knot is tied in
the same fashion as in the continuous simple suture.
84.
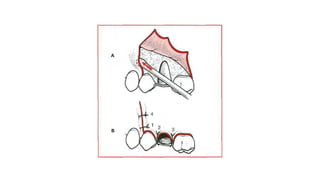
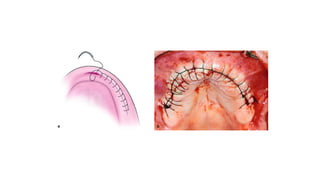
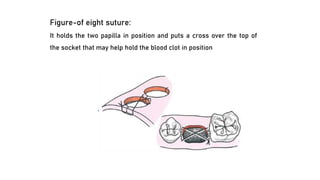
Figure-of eight suture:
Itholds the two papilla in position and puts a cross over the top of
the socket that may help hold the blood clot in position
Most intraoral suturesare tied with surgeon’s knot:
A, Suture is pulled through tissue until short tail of suture
(approximately 15 to 20 mm long) remains. Needle holder is held
horizontally by right hand in preparation for knot-tying procedure.
B, Left hand then wraps long end of suture around needle holder
twice in clockwise direction to make two loops of suture around
needle holder.
C, Surgeon then opens needle holder and grasps short end of suture
near its end.
D , Ends of suture are then pulled to tighten knot. Needle holder
should not pull suture at all until knot is nearly tied, to avoid
lengthening that portion of suture.
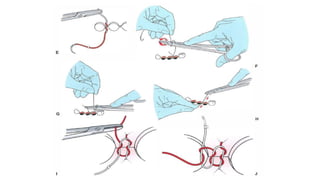
89.
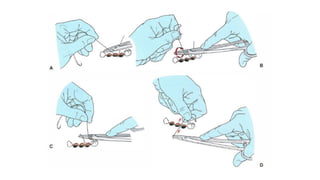
E, End offirst step of surgeon's knot. The double wrap has resulted in double
overhand knot. This increases friction in knot and will keep wound edges
together until second portion of knot is tied.
F, Needle holder is then released from short end of suture and held in same
position as when knot-tying procedure began. Left hand then makes Single wrap
in counterclockwise direction.
G, Needle holder then grasps short end of suture at its end.
H, This portion of knot is completed by pulling this loop firmly down against
previous portion of knot.
I, This completes surgeon's knot. Double loop of first pass holds tissue together
until second portion of square knot can be tied.
J, Most surgeons add third throw to their instrument tie when using a resorbable
material. Needle holder is repositioned in original position, and one wrap is
placed around needle holder in original clockwise direction. Short end of suture is
grasped and tightened down firmly to form second square knot. Final throw of
three knots is tightened firmly.





































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




