Downloaded 256 times























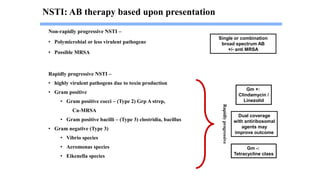








Necrotizing fasciitis is a life-threatening, rapidly spreading infection that destroys skin and soft tissue, primarily caused by bacteria such as group A streptococcus. It presents with flu-like symptoms, swelling, and rapidly progresses to critical states including necrosis and septic shock if not diagnosed and treated promptly with surgical debridement and antibiotics. Early intervention and appropriate management are crucial for survival, with a significant mortality rate if left untreated.













































































