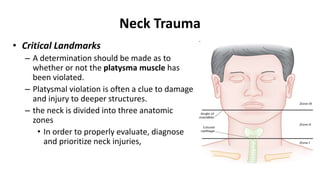
This document discusses neck trauma, focusing on evaluation and management in the emergency department. It divides the neck into 3 zones based on anatomical structures. Zone I injuries carry the highest risk but are difficult to access. Zone II injuries are most common and can often be explored surgically with low morbidity. Zone III injuries are also surgically challenging. Evaluation may involve imaging like C-spine films, CT, or angiography. Unstable patients generally require immediate surgery. Stable patients can often be managed with selective diagnostic tests to determine if surgery is needed.