Learning objectives
At theend of the session the participants will be able to:
Enlist mechanism of injury in trauma
Understand about various
Thoracic injuries
Abdominal injuries
Fractures
Complications of trauma
Blunt:
Common in
Motor vehiclecrash
Contact sports
Assault with blunt objects
Fall from height.
Severity depends on the amount of kinetic
energy dissipated to the body and underlying
structures.
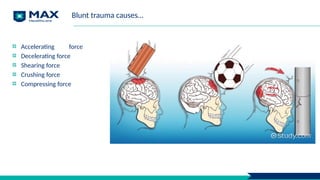
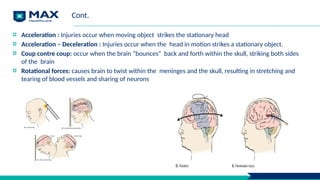
Cont.
Acceleration : Injuriesoccur when moving object strikes the stationary head
Acceleration – Deceleration : Injuries occur when the head in motion strikes a stationary object.
Coup contre coup: occur when the brain “bounces” back and forth within the skull, striking both sides
of the brain
Rotational forces: causes brain to twist within the meninges and the skull, resulting in stretching and
tearing of blood vessels and sharing of neurons
8.
Prehospital resuscitation
Goal: Immediatestabilization and transportation.
Airway maintenance
Control of external bleeding and shock
Immobilization
Immediate transport
Based on Advanced Trauma Life Support (ATLS)
9.
Primary evaluation andmanagement
Primary survey:
Airway assessment and protection - maintain cervical spine stabilization when appropriate
Breathing and ventilation assessment - maintain adequate oxygenation
Circulation - control hemorrhage and maintain adequate end-organ perfusion
Disability - perform basic neurologic evaluation
Exposure with environmental control - undress patient and search everywhere for possible injury,
while preventing hypothermia.
10.
Points to rememberedduring primary survey
Airway obstruction is a major cause of death immediately following trauma
Intubate When in doubt, it is generally best to intubate early, particularly in patients with hemodynamic
instability, or those with significant injuries to the face or neck, which may lead to swelling and
distortion of the airway
Secure airway after intubation
Unconscious patients with small pneumothoraces that are not visible or missed on the initial chest
radiograph
It is important to reauscultate the lungs of trauma patients who develop hemodynamic instability after
being intubated.
Be alert for subtle signs of hemorrhagic shock, particularly in the elderly and young, healthy adults who
may not present with obvious manifestations.
Brain injuries are common in patients who have sustained severe blunt trauma
11.
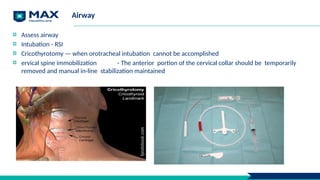
Airway
Assess airway
Intubation -RSI
Cricothyrotomy — when orotracheal intubation cannot be accomplished
ervical spine immobilization - The anterior portion of the cervical collar should be temporarily
removed and manual in-line stabilization maintained
12.
RSI – preparationSOAPME
Suction Oxygen Airways
ET tube
Stylet
—Laryngoscope- Blade – Mac 3 or 4 for adults, Miller
—video laryngoscope, LMA and bougie at bedside
Pre-oxygenate – 15 LPM NRBM
Monitoring equipment/Medications
End Tidal CO2
13.
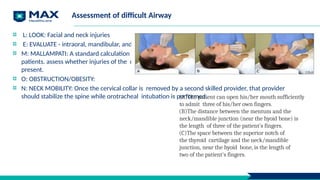
Assessment of difficultAirway
L: LOOK: Facial and neck injuries
E: EVALUATE - intraoral, mandibular, and hyoid-to- thyroid notch distances.
M: MALLAMPATI: A standard calculation of the Mallampati score cannot be performed in many trauma
patients. assess whether injuries of the oropharynx or pooled blood, vomitus, or secretions are
present.
O: OBSTRUCTION/OBESITY:
N: NECK MOBILITY: Once the cervical collar is removed by a second skilled provider, that provider
should stabilize the spine while orotracheal intubation is performed.
(A)The patient can open his/her mouth sufficiently
to admit three of his/her own fingers.
(B)The distance between the mentum and the
neck/mandible junction (near the hyoid bone) is
the length of three of the patient's fingers.
(C)The space between the superior notch of
the thyroid cartilage and the neck/mandible
junction, near the hyoid bone, is the length of
two of the patient's fingers.
14.
Recognition of thedifficult airway
Grade I: Fully visible tonsils,
Uvula, soft palate Grade II:
Visible hard and soft palate,
upper portion of tonsil and
uvula
Grade III: Visible Soft and
hard palate and base of the
uvula.
Grade IV: Only hard palate
visible
15.
Resuscitation
Aimed at ensuringadequate perfusion of tissues
Large bore peripheral IV catheters
Draw blood samples
IV: Crystalloid
Blood transfusion
Gastric and urinary catheter placement.
16.
Secondary survey:
Begins afterresuscitation is well established and vital signs are normalized
History
Head to toe examination
Completion of special procedures – ECG, X-rays, USG
Monitor vitals
Definitive Care/ operative phase: Depending on type of injury Critical care phase:
Ongoing physical assessment
Monitoring patients response for treatment
Maintain oxygenation
Prevention of complications
17.
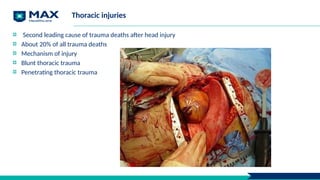
Thoracic injuries
Second leadingcause of trauma deaths after head injury
About 20% of all trauma deaths
Mechanism of injury
Blunt thoracic trauma
Penetrating thoracic trauma
Rib Fracture
Most commonchest injury
Most commonly 5th to 9th ribs
1st and 2nd rib – Intrathoracic vascular injuries
Fractures of 8th to 12th ribs can damage underlying abdominal solid organs:
Liver
Spleen
Kidneys
Signs and Symptoms
Localized pain, tenderness.
Pain Increases on Coughs, Moves and Breathes deeply
Chest wall instability
Deformity, discoloration
Associated pneumo or hemothorax
19
20.
Diagnosis:
Chest X ray,clinical examination
Management:
Depends on no. of ribs fractured, degree of underlying injury, and age of the patient.
High concentration O2
Splinting.
Pain control
Encourage patient to breath deeply
21.
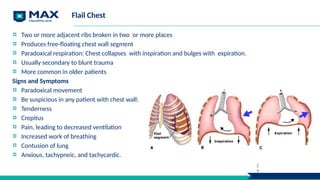
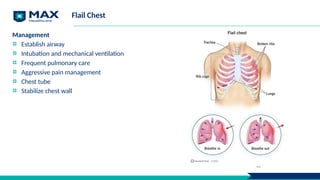
Flail Chest
Two ormore adjacent ribs broken in two or more places
Produces free-floating chest wall segment
Paradoxical respiration: Chest collapses with inspiration and bulges with expiration.
Usually secondary to blunt trauma
More common in older patients
Signs and Symptoms
Paradoxical movement
Be suspicious in any patient with chest wall:
Tenderness
Crepitus
Pain, leading to decreased ventilation
Increased work of breathing
Contusion of lung
Anxious, tachypneic, and tachycardic.
2
9
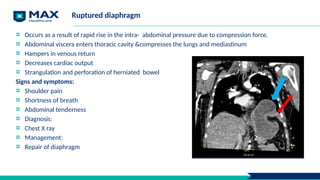
Ruptured diaphragm
Occurs asa result of rapid rise in the intra- abdominal pressure due to compression force.
Abdominal viscera enters thoracic cavity &compresses the lungs and mediastinum
Hampers in venous return
Decreases cardiac output
Strangulation and perforation of herniated bowel
Signs and symptoms:
Shoulder pain
Shortness of breath
Abdominal tenderness
Diagnosis:
Chest X ray
Management:
Repair of diaphragm
24.
Pulmonary injuries
Pulmonary contusions:
Mayoccur unilateral / bilateral
Manifested as hemorrhage and then edema
Inflammation affects alveolar capillary units.
Leads to decrease compliance
Increased pulmonary vascular resistance
Decreased blood flow.
Ventilation perfusion imbalances.
Symptoms may develop after 24 to 48 hours
Ecchymosis of chest wall
Crackles in contused lung
Cough with blood- tinged sputum
Poor lung function -Systemic arterial hypoxemia
25.
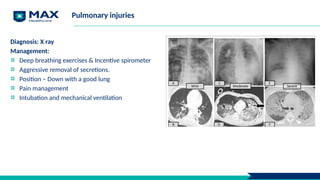
Pulmonary injuries
Diagnosis: Xray
Management:
Deep breathing exercises & Incentive spirometer
Aggressive removal of secretions.
Position – Down with a good lung
Pain management
Intubation and mechanical ventilation
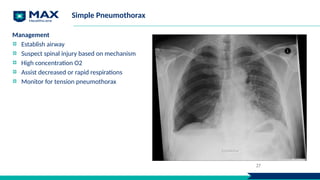
26.
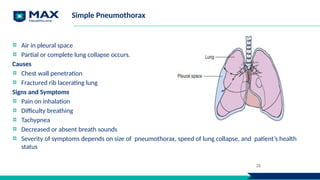
Simple Pneumothorax
Air inpleural space
Partial or complete lung collapse occurs.
Causes
Chest wall penetration
Fractured rib lacerating lung
Signs and Symptoms
Pain on inhalation
Difficulty breathing
Tachypnea
Decreased or absent breath sounds
Severity of symptoms depends on size of pneumothorax, speed of lung collapse, and patient’s health
status
26
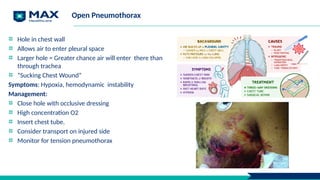
Open Pneumothorax
Hole inchest wall
Allows air to enter pleural space
Larger hole = Greater chance air will enter there than
through trachea
“Sucking Chest Wound”
Symptoms: Hypoxia, hemodynamic instability
Management:
Close hole with occlusive dressing
High concentration O2
Insert chest tube.
Consider transport on injured side
Monitor for tension pneumothorax
28
29.
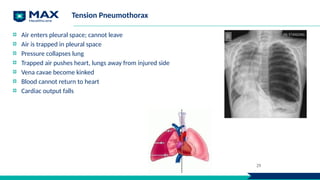
Tension Pneumothorax
Air enterspleural space; cannot leave
Air is trapped in pleural space
Pressure collapses lung
Trapped air pushes heart, lungs away from injured side
Vena cavae become kinked
Blood cannot return to heart
Cardiac output falls
29
30.
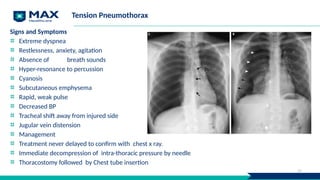
Tension Pneumothorax
Signs andSymptoms
Extreme dyspnea
Restlessness, anxiety, agitation
Absence of breath sounds
Hyper-resonance to percussion
Cyanosis
Subcutaneous emphysema
Rapid, weak pulse
Decreased BP
Tracheal shift away from injured side
Jugular vein distension
Management
Treatment never delayed to confirm with chest x ray.
Immediate decompression of intra-thoracic pressure by needle
Thoracostomy followed by Chest tube insertion
30
31.
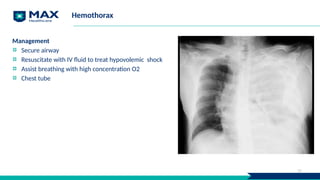
Hemothorax
Blood in pleuraspace
Most common result of major chest wall trauma
Present in 70 to 80% of penetrating, major non-penetrating chest trauma
Signs and Symptoms
Decreased breath sounds
Dull to percussion on affected side
Rapid, weak pulse
Cool, clammy skin
Restlessness, anxiety
Thirst
Hypotension
Collapsed neck veins
Respiratory distress
Shock precedes ventilatory failure
31
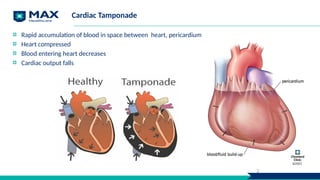
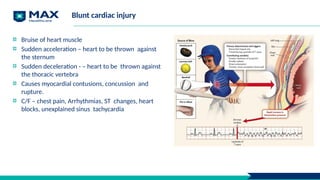
Blunt cardiac injury
Bruiseof heart muscle
Sudden acceleration – heart to be thrown against
the sternum
Sudden deceleration - – heart to be thrown against
the thoracic vertebra
Causes myocardial contusions, concussion and
rupture.
C/F – chest pain, Arrhythmias, ST changes, heart
blocks, unexplained sinus tachycardia
38.
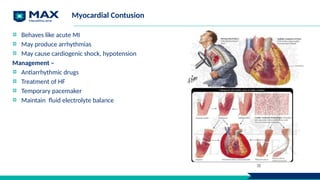
Myocardial Contusion
Behaves likeacute MI
May produce arrhythmias
May cause cardiogenic shock, hypotension
Management –
Antiarrhythmic drugs
Treatment of HF
Temporary pacemaker
Maintain fluid electrolyte balance
38
39.
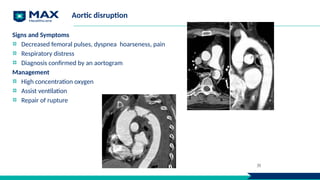
Aortic disruption
Signs andSymptoms
Decreased femoral pulses, dyspnea hoarseness, pain
Respiratory distress
Diagnosis confirmed by an aortogram
Management
High concentration oxygen
Assist ventilation
Repair of rupture
39
Nursing management
Ineffective tissueperfusion – Oxygen administration, blood transfusion,
Pain – Analgesics, bed rest
Risk for infection – Care of fixators, dressing
Risk for injury – Neurovascular assessment,
42.
Complications of trauma
Hypermetabolism : Due to metabolic response to injury.
Infection
Sepsis
Pulmonary
Respiratory failure
Fat embolism syndrome
Pain
Renal complications:
Renal failure
Myoglobinuria
Vascular complications
Compartment syndrome
DVT
Missed injuries
MODS
43.
Role of ICUNurses In
Management of other Emergency
Conditions (Drug Overdose &
Poisoning)
44.
Learning Objective
At theend of the session learner will be able to:
To illustrate clinical manifestation & how to manage & facilitate nursing care to the patient with drug overdose.
To have concise knowledge of the general line of treatment to be followed if a case of poisoning.
45.
Drug Overdose
A drugoverdose occurs when a person consumes an excessive amount of a drug, whether it is prescribed, over-
the-counter or illicit drugs.
It can be accidental or intentional and can occur from taking too much of a drug at once or over a prolonged
period.
Overdoses can affect different systems in the body, such as the respiratory system, central nervous system, and
cardiovascular system.
Depending on the type and amount of drug consumed, the symptoms of an overdose can vary widely.
46.
Risk factors
Improper storageof drugs
Recreation
Not knowing or following
dosage instructions
History of mental disorders
History of misuse or addiction
47.
Signs & symptoms
Shallowor slow breathing
Blue or pale skin
Pinpoint pupils
Nausea or vomiting
Dizziness or confusion
Seizures
Loss of consciousness
48.
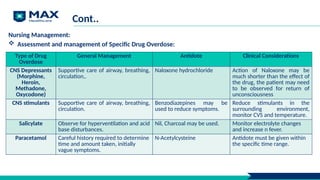
Cont..
Nursing Management:
Assessmentand management of Specific Drug Overdose:
Type of Drug
Overdose
General Management Antidote Clinical Considerations
CNS Depressants
(Morphine,
Heroin,
Methadone,
Oxycodone)
Supportive care of airway, breathing,
circulation,.
Naloxone hydrochloride Action of Naloxone may be
much shorter than the effect of
the drug, the patient may need
to be observed for return of
unconsciousness
CNS stimulants Supportive care of airway, breathing,
circulation.
Benzodiazepines may be
used to reduce symptoms.
Reduce stimulants in the
surrounding environment,
monitor CVS and temperature.
Salicylate Observe for hyperventilation and acid
base disturbances.
Nil, Charcoal may be used. Monitor electrolyte changes
and increase n fever.
Paracetamol Careful history required to determine
time and amount taken, initially
vague symptoms.
N-Acetylcysteine Antidote must be given within
the specific time range.
49.
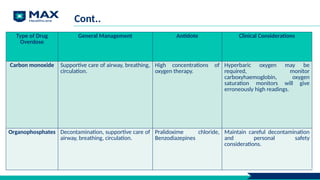
Cont..
Type of Drug
Overdose
GeneralManagement Antidote Clinical Considerations
Carbon monoxide Supportive care of airway, breathing,
circulation.
High concentrations of
oxygen therapy.
Hyperbaric oxygen may be
required, monitor
carboxyhaemoglobin, oxygen
saturation monitors will give
erroneously high readings.
Organophosphates Decontamination, supportive care of
airway, breathing, circulation.
Pralidoxime chloride,
Benzodiazepines
Maintain careful decontamination
and personal safety
considerations.
50.
Management of Drugover dose
The management of drug overdose depends on the type and amount of drug consumed, the severity of the
symptoms, and the time since ingestion. Here are some general steps that may be taken in managing a drug
overdose:
Call for emergency medical assistance: Time is critical in managing drug overdose, and delaying treatment can
lead to serious complications or death.
Assess the person's condition: Check the person's breathing, pulse, and level of consciousness. If the person is
unresponsive, start cardiopulmonary resuscitation (CPR) immediately.
51.
Management of Drugover dose
Provide first aid: If the person is conscious and breathing, try to keep them calm and comfortable. Remove any
drugs or drug paraphernalia from the person's surroundings. If the person is vomiting, turn them on their side to
prevent choking.
Obtain proper history: The type of drug consumed, the amount, and the time of ingestion. This information can
help to determine the appropriate treatment.
Administer medication: Depending on the drug consumed, appropriate.
Provide supportive care: Such as monitoring vital signs, providing oxygen therapy, or giving intravenous fluids.
52.
Intensive care managementof drug overdose
The goal is to provide comprehensive care that addresses both the physical and psychological needs of the patient.
Continuous monitoring: close monitoring of vital signs, including heart rate, blood pressure, respiratory rate,
and oxygen saturation.
Stabilization: The immediate goal of intensive care management is to stabilize the patient's condition. This may
involve administering medication to reverse the effects of the drug, such as naloxone for opioid overdose, or
providing supportive care, such as oxygen therapy or intravenous fluids.
Airway management: In some cases, patients may require intubation and mechanical ventilation to maintain
their airway and support breathing.
53.
Intensive care managementof drug overdose
Gastric decontamination: It may be necessary to remove any remaining drug from the patient's stomach. This
may involve inducing vomiting, administering activated charcoal, or performing gastric lavage.
Management of complications: Including seizures, respiratory failure, and cardiac arrest.
Providing advanced life support measures in case of cardiac arrest.
Psychological support: To help them cope with the aftermath of the overdose and prevent future occurrences.
It's important to note that the intensive care management of drug overdose is a complex and multifaceted
process that requires a team approach involving medical professionals from multiple disciplines, including critical
care specialists, toxicologists, and psychologists.
Poisoning
A condition wherea person is harmed due to the ingestion, inhalation, injection, or absorption of toxic
substances into the body.
It can be accidental, intentional, or occupational.
The symptoms and severity of poisoning depend on the type and amount of the toxic substance, the route of
exposure, and the individual's age, health, and metabolism.
Some common examples of poisoning include ingestion of household chemicals or medications, exposure to
pesticides or industrial chemicals, ingestion of contaminated food or water, and accidental or intentional
overdose of drugs or alcohol.
56.
Symptoms
The symptoms ofpoisoning can vary widely,
but common signs include
Nausea
Vomiting
Diarrhea
Abdominal pain
Difficulty breathing
Confusion
Dizziness
Seizures
Unconsciousness.
If you suspect someone is poisoned, it is
important to seek emergency medical
attention immediately.
57.
Management of Poisoning
Themanagement of poisoning in the ICU (Intensive Care Unit) involves several steps:
Stabilization: The first step is to stabilize the patient's vital signs, such as blood pressure, heart rate, and oxygen
saturation. This may involve administering fluids, oxygen, or medications to treat symptoms such as seizures,
agitation, or respiratory distress.
Identification: The next step is to identify the toxic substance responsible for the poisoning, if possible. This may
involve obtaining a history of the patient's exposure, performing laboratory tests or imaging studies, or
consulting with a toxicologist.
Elimination: Once the toxic substance has been identified, steps can be taken to eliminate it from the patient's
body. This may involve administering antidotes, performing dialysis or other forms of extracorporeal therapy, or
supporting the patient's natural detoxification processes.
58.
Cont.
Supportive Care: Thepatient may require supportive care such as mechanical ventilation, continuous
renal replacement therapy, or monitoring of electrolyte imbalances.
Prevention of Complications: Patients with poisoning are at risk of developing complications such as
pneumonia, sepsis, or organ failure. Therefore, it is important to closely monitor the patient's condition
and address any complications that arise.
Rehabilitation: Once the patient has recovered from the acute phase of poisoning, rehabilitation may
be required to help them regain strength and function.
The management of poisoning in the ICU requires a multidisciplinary approach, involving toxicologists, critical care physicians,
nurses, and other healthcare professionals. Close monitoring and prompt intervention can help improve outcomes for patients
with poisoning.
Physical Care
Identify and
observe
Identifyand observe for the effects of more than one substance in
every intoxicated person
Ensure Ensure thorough physical and mental status examination
Measure Measure fluid intake and maintain hydration
Maintain Maintain observations half hourly in the acute phase and then 2nd
hourly until stable
Take Take baseline observations: blood pressure, respiratory rate,
temperature and pulse
61.
Behavioral Management
Guidelines ForManagement Of Specific Behaviours
Of An Intoxicated Patient
Anxiety, agitation, panic Approach in a calm and confident manner
Explain interventions
Move and speak in an unhurried way
Minimise the number of staff attending to the patient
Provide a quiet environment to reduce stimulation
Reassure the patient frequently
Protect the patient from accidental harm
Confusion, disorientation Use clear and simple communication
Provide frequent reality orientation
Display some object familiar to the patient, for example- own dressing gown
or slippers
Ensure frequent supervision
Accompany the patient to and from places (e.g. bathroom, TV lounge)
62.
Cont.
Guidelines For ManagementOf Specific Behaviours
Of An Intoxicated Patient
Altered perception,
hallucinations
Explain perceptual errors and re-orientate
Create a simple, uncluttered environment
Nurse in well-lit surroundings to avoid perceptual confusion
Protect the patient from harm
Anger, aggression Use space for self-protection (e.g. don’t crowd the patient, keep furniture
between yourself and the patient if feeling unsafe)
Speak in a calm, reassuring way
Use the patient’s name when speaking to them
Do not challenge or threaten the patient by tone of voice, eyes or body
language
Let the patient air their feelings, and acknowledge them
Determine the source of the patient’s anger and if possible, remove it
Be flexible within reason
Be aware of workplace policies on managing aggression
Basic Sepsis LifeSupport (BSLS)
Our Vision: Improve the lives of our sepsis patients, families, and educate skilled healthcare
professionals, and conduct training that expands clinical knowledge
Our Goal : Early detection and treatment of sepsis and septic shock to reduce sepsis mortality
65.
Learning objectives
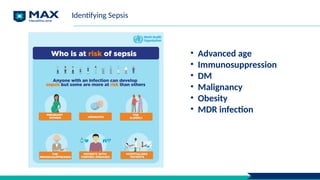
• Torecognize patients that require sepsis screening – high risk groups,
deterioration due to infection & those with signs of sepsis
• To define sepsis & septic shock and document same
• To know when & how to use the Adult Sepsis pathway to aid recognition and
treatment
• To implement with 1 hour sepsis bundle
• To Identify when to escalate care
66.
Step1 :Sepsis Recognition
Step2: Focused examination and Assessment
Step 3: One hour Bundle
Step 4 : Monitoring goals of sepsis
Step 5: Infection control practises, source control and
ID consult
Step 6: Disposition
Six steps of sepsis management
67.
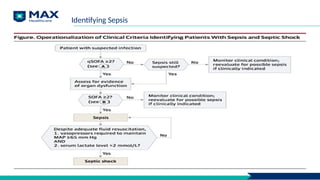
Sepsis: Defining =Identifying
= life-threatening organ dysfunction
➡ caused by a dysregulated host response
➡to infection
= a life-threatening condition
➡ when the body’s response to an infection
➡injures its own tissues and organs
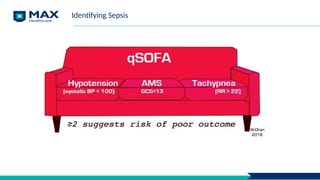
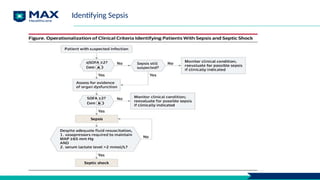
Identifying Sepsis
68.
Continuum of severity(SIRS not included)
Identifying Sepsis
Infection
Bacteraemi
a
Sepsis
Septic
shock
69.
Identifying Sepsis
Septic Shock:Defining = Identifying
Sepsis PLUS
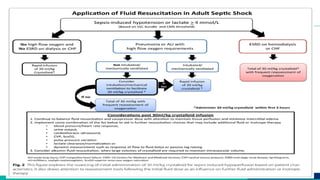
➡ Persistent hypotension*** requiring vasopressors to maintain MAP >/= 65
AND
➡ Lactate >/= 2 mmol/L
***despite adequate volume resuscitation
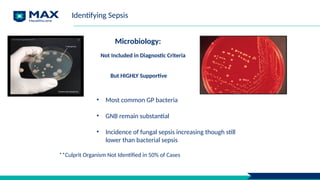
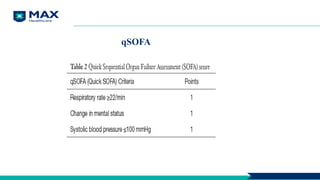
Microbiology:
Not Included inDiagnostic Criteria
But HIGHLY Supportive
**Culprit Organism Not Identified in 50% of Cases
• Most common GP bacteria
• GNB remain substantial
• Incidence of fungal sepsis increasing though still
lower than bacterial sepsis
Identifying Sepsis
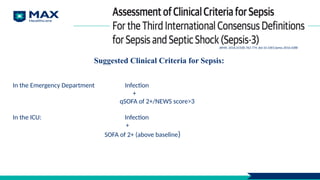
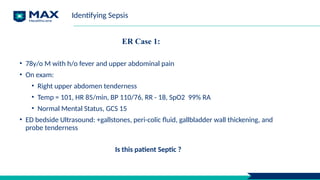
ER Case 1:
•78y/o M with h/o fever and upper abdominal pain
• On exam:
• Right upper abdomen tenderness
• Temp = 101, HR 85/min, BP 110/76, RR - 18, SpO2 99% RA
• Normal Mental Status, GCS 15
• ED bedside Ultrasound: +gallstones, peri-colic fluid, gallbladder wall thickening, and
probe tenderness
Is this patient Septic ?
Identifying Sepsis
ER Case cont:
•78 y/o M with h/o Fever, Upper Abdominal Pain and
decreased urination x 1 day
• On exam:
• Right upper abdomen Tenderness
• Temp = 101, HR 110, BP 110/76, RR = 26, SpO2
90% on RA
• GCS = 12, confused
• ED bedside Ultrasound: +gallstones, peri-colic fluid,
gallbladder wall thickening, and probe tenderness
• ABG suggestive of hypoxia ( PaO2 - 55 mm of Hg in
room air)
• Normal lactate
What is your diagnosis now - is this patient is septic?
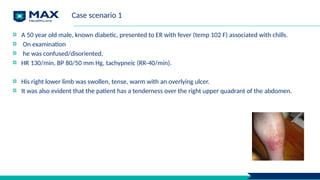
Case scenario 1
A50 year old male, known diabetic, presented to ER with fever (temp 102 F) associated with chills.
On examination
he was confused/disoriented,
HR 130/min, BP 80/50 mm Hg, tachypneic (RR-40/min).
His right lower limb was swollen, tense, warm with an overlying ulcer.
It was also evident that the patient has a tenderness over the right upper quadrant of the abdomen.
88.
Why investigate?
To identifycausative agent
To evaluate organ dysfunction
To identify source of infection
To aid prognosis and selection of appropriate level of care
89.
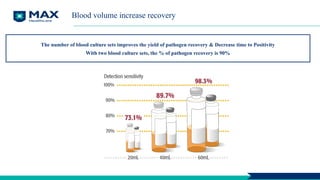
Blood volume increaserecovery
The number of blood culture sets improves the yield of pathogen recovery & Decrease time to Positivity
With two blood culture sets, the % of pathogen recovery is 90%
Case continued
HR135/min, RR 35/min, BP 76/44 mmHg
PaO2 50, mixed acidosis, lactate 6
20 ml/kg RL in 1h, C/S sent, B/L diffuse infiltrates
NE infused, Intubated & ventilated (persistent
shock/hypoxemia)
Persisting tachycardia & hypotension
96.
What will bethe best step
Another bolus of 15-20 ml/kg fluid
NE/add vasopressin
CVP Guided therapy
Dynamic parameters guided therapy
97.
Tissue perfusion &organ support
Prevent iatrogenic damage (eg. excess
fluids, volutrauma)
Facilitate source control
Involve family for goals of care and
prognosis
What are we aiming for?
MAP >65 mmHg
SpO2 >88–90%
Pplat <30 cm H2O
Urine output – 0.5-1ml/kg/h
Decrease in lactates
Maintaining adequate perfusion
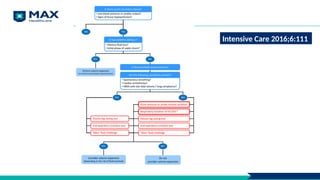
Document reassessment ofvolume status and tissue perfusion
EITHER repeat focused exam (after initial fluid resuscitation)
Vital signs, cardiopulmonary status, capillary refill, pulse, and skin findings.
Two of the following:
Bedside cardiovascular ultrasound
Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge
Measure CVP
Measure ScvO2
100.
Monitoring infection control
Contactprecautions /Negative and Positive Isolation
Repeat culture only for fungal growth to decide on therapy duration
For Staph aureus, r/o vegetations, prosthesis
Drain empyema/ascitic fluid in SBP, remove lines/tubes, debride wounds
101.
Reassessment during monitoring
Animportant marker of global organ perfusion: Lactate
After resuscitation, monitor all organ systems
Fluid therapy guided both by fluid responsiveness & tolerance
Assess & control infection