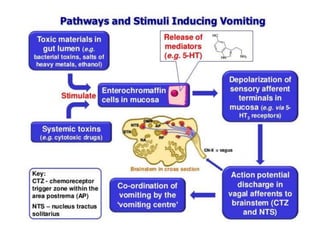
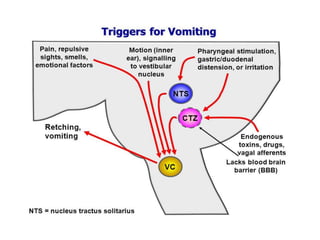
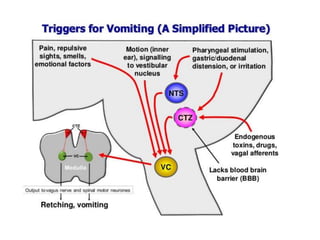
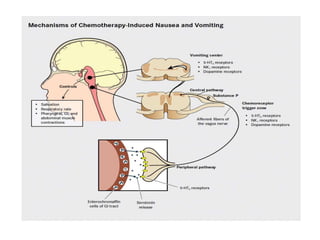


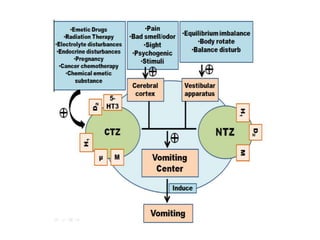
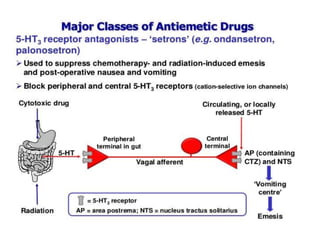

The document discusses nausea and vomiting, defining emetics as agents that induce vomiting primarily used in poisoning cases. It outlines the mechanisms and pathways involved in the vomiting process, highlighting the roles of the vomit center in the medulla oblongata and neurotransmitter receptors. It also emphasizes the management strategies for nausea and vomiting, including pharmacological and non-pharmacological treatments, and the critical role of pharmacists in monitoring and referring patients when necessary.








































![[Pharma] vomiting and anti emetics](https://cdn.slidesharecdn.com/ss_thumbnails/pharmavomitingandanti-emetics-150502144626-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)














































