1) The document discusses an approach to evaluating muscle weakness by differentiating true muscle weakness from fatigue or functional weakness. It provides a classification and diagnostic algorithm.
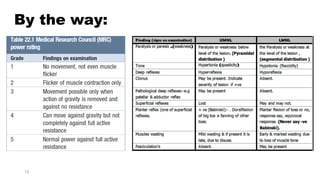
2) Key points in the evaluation include determining if weakness is objective or subjective, localized or generalized, and distinguishing upper motor neuron from lower motor neuron signs.
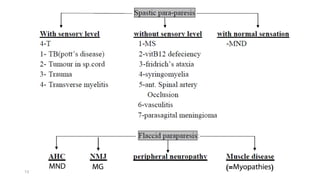
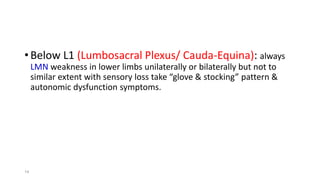
3) Differential diagnoses discussed include myopathies, motor neuron diseases, neuropathies, stroke, spinal cord lesions, multiple sclerosis, myasthenia gravis, and functional causes.
4) An algorithm is provided that approaches weakness by determining acuity and characteristics to guide appropriate testing and potential referrals.
![• Fatigue is subjective term reported by patient as weakness-like
complain felt after exercise but actually muscle power is normal, i.e:
no pathology in muscle or in its nerve supply. So fatigue is non-
objective muscle weakness, non-neuromuscular weakness,
functional muscle weakness or false muscle weakness.
Motor Nerve Supply
True Muscle Weakness
Wrong neither in
muscle nor in its
nerve supply
Functional
Muscle
weakness
[Myopathy]Muscle
3](https://image.slidesharecdn.com/approachtomuscleweakness-181006003422/85/Approach-to-muscle-weakness-3-320.jpg)