Downloaded 79 times

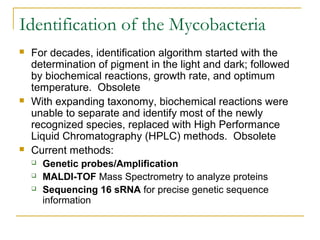










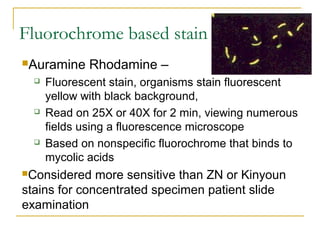
![Acid Fast staining of the Mycobacteria
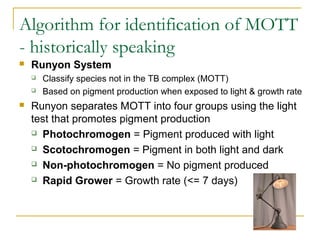
Mycobacterium avium complex
Organisms are routinely shorter than TB
(Kinyoun stain) No cording
M. Tuberculosis - Organisms are
long rods and can appear as if they
are sticking together [cord factor]
In broth
cultures -
ropes of TB
will form due to
cord factor](https://image.slidesharecdn.com/websitemycobacteriologyupdate2018-180410013845/85/Mycobacteriology-Update-2018-21-320.jpg)









![Mycobacterium bovis
Produces disease in cattle and other animals
Spread to humans by raw milk ingestion
Disease in humans similar to that caused by TB
Bladder infections in patients treated with BCG [Bacille Calmette-
Guerin] when used as an immune adjuvant to treat bladder cancer
BCG is an attenuated strain of M. bovis
It can become “active” and infect the bladder
M. bovis will be isolated from urine specimens
Is it M bovis or is it M tb?
M.bovis M. tb
Nitrate Negative Positive
Growth in T2H* No growth Growth
Pyrazinamidase Negative Positive
*(Thiophene-2-carboxylic hydrazide)](https://image.slidesharecdn.com/websitemycobacteriologyupdate2018-180410013845/85/Mycobacteriology-Update-2018-32-320.jpg)














This document provides an overview of mycobacteriology and tuberculosis. It discusses the characteristics of acid-fast bacilli including their cell walls and staining properties. Current methods for identifying mycobacteria include genetic probes, MALDI-TOF mass spectrometry, and 16S rRNA sequencing. There are over 170 recognized mycobacterial species, including those in the TB complex like M. tuberculosis, as well as many non-tuberculosis mycobacteria. Proper specimen collection, processing, staining, culturing, and molecular/genetic techniques are required for accurate identification and diagnosis of mycobacterial infections.























































































