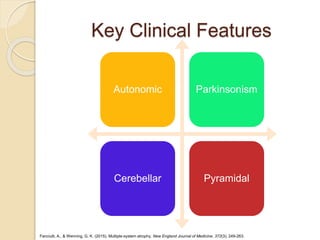
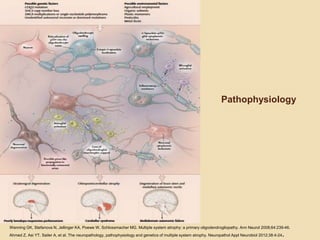
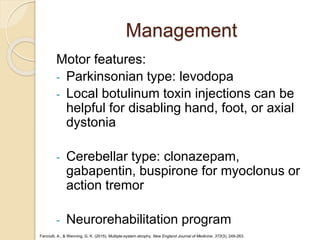
Multiple system atrophy is a rare, fatal neurodegenerative disease characterized by parkinsonian or cerebellar features and autonomic dysfunction. It is caused by the accumulation of alpha-synuclein protein in oligodendrocytes throughout the brain and spinal cord. There are no disease-modifying treatments available, so management focuses on alleviating motor symptoms and addressing problems related to autonomic failure and other non-motor issues.

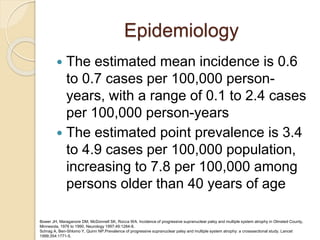
![Diagnostic Criteria
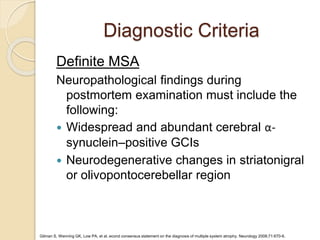
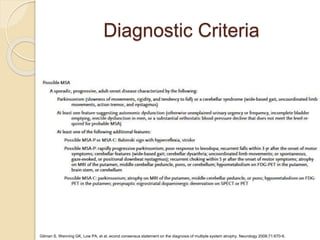
Probable MSA
Sporadic, progressive disease in adults (onset after 30 yr
of age) characterized by autonomic failure, including
urinary incontinence (with erectile dysfunction in men),
or an orthostatic decrease in blood pressure by at least
30 mm Hg systolic or 15 mm Hg diastolic within 3 min of
standing, plus one of the following:
Parkinsonism (slowness of movements, rigidity, and
tendency to fall) with poor response to levodopa
(parkinsonian subtype [MSA-P])
A cerebellar syndrome (wide-based gait, uncoordinated
limb movements, action tremor, and nystagmus)
(cerebellar subtype [MSA-C])
Gilman S, Wenning GK, Low PA, et al. econd consensus statement on the diagnosis of multiple system atrophy. Neurology 2008;71:670-6.](https://image.slidesharecdn.com/multiplesystematrophy0118-180124141754/85/Multiple-System-Atrophy-13-320.jpg)










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















