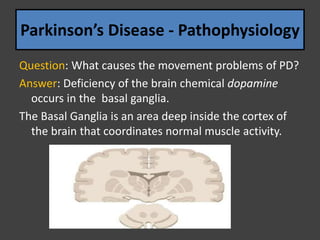
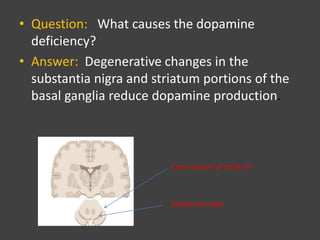
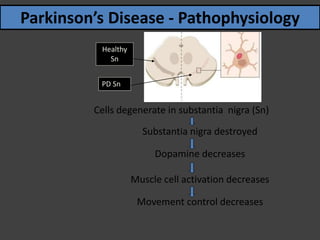
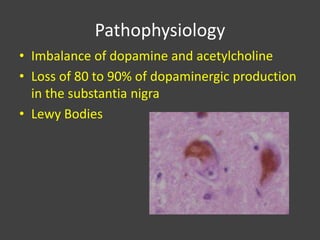
Parkinsonism is a clinical syndrome characterized by symptoms such as tremors, rigidity, and bradykinesia, first described by James Parkinson in 1817 and more commonly seen in individuals over 65 years old. The disease is primarily linked to dopamine deficiency due to degeneration in the substantia nigra, leading to impaired motor control and various other symptoms, including cognitive decline. Multiple System Atrophy (MSA) is a progressive disorder with features of parkinsonism and autonomic dysfunction, distinguished into two categories based on predominant symptoms.