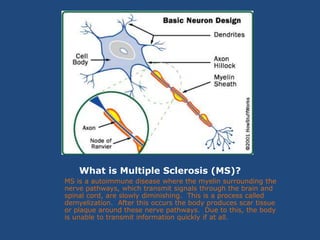
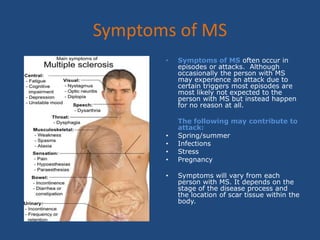
Multiple sclerosis (MS) is an autoimmune disease that causes demyelination of nerve pathways in the brain and spinal cord, impairing signal transmission. There are four stages of MS: relapsing-remitting, secondary progressive, primary progressive, and progressive-relapsing. Symptoms vary by individual but may include fatigue, tremors, cognitive changes, sensory deficits, weakness, and mobility issues. Occupational therapy can help people with MS through fatigue management, controlling tremors, cognitive compensation strategies, improving sensory function, strength and endurance training, contracture prevention, improving activities of daily living, and use of adaptive equipment.