Download as PDF, PPTX

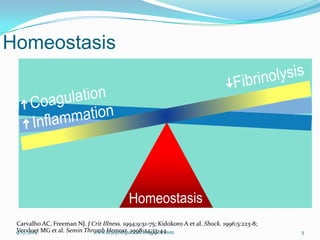
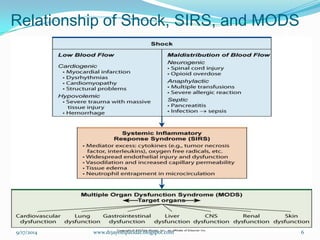
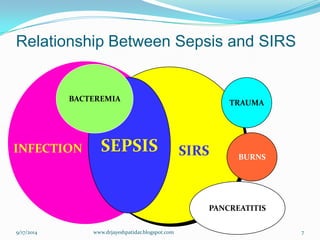
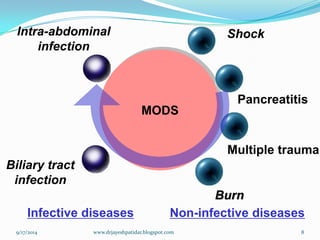
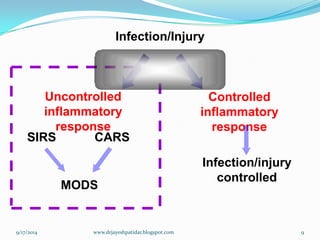
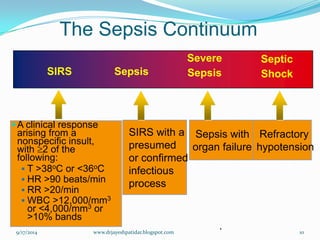
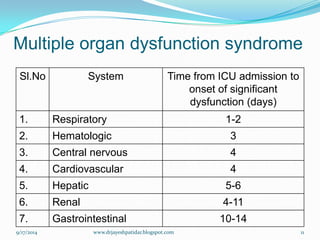
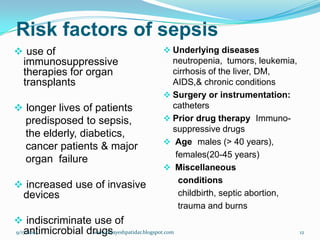
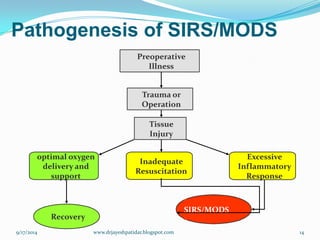
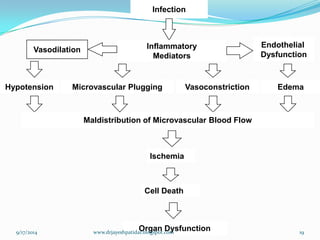
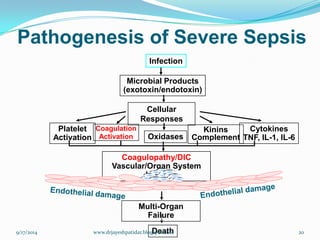
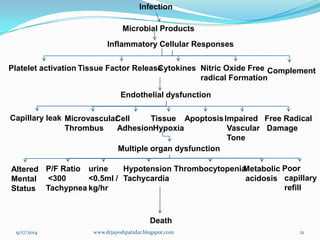
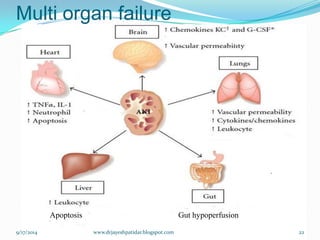


The document discusses sepsis, SIRS, and MODS (multiple organ dysfunction syndrome). It defines sepsis as the systemic response to infection, SIRS as the inflammatory response to various insults, and MODS as altered organ function in an acutely ill patient that cannot be maintained without intervention. The relationships between sepsis, SIRS, and MODS are explained, along with their pathogenesis and potential complications like respiratory distress and multi-organ failure. Risk factors, diagnosis, management goals, and nursing interventions are also outlined.