This document discusses sepsis, including its definition, causes, pathophysiology, clinical features, treatment, and research. The key points are:
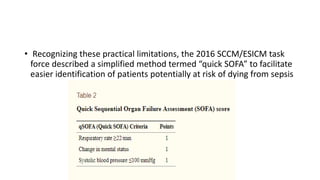
- Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. It is divided into sepsis and septic shock.
- Common causes are pneumonia, abdominal/urinary infections. Risk factors include chronic diseases and older/younger age.
- Pathophysiology involves a complex host response involving both pro- and anti-inflammatory mechanisms that can lead to organ dysfunction.
- Treatment focuses on early management bundles within 6 hours including antibiotics, fluids, vasopressors, and source control, as well as organ