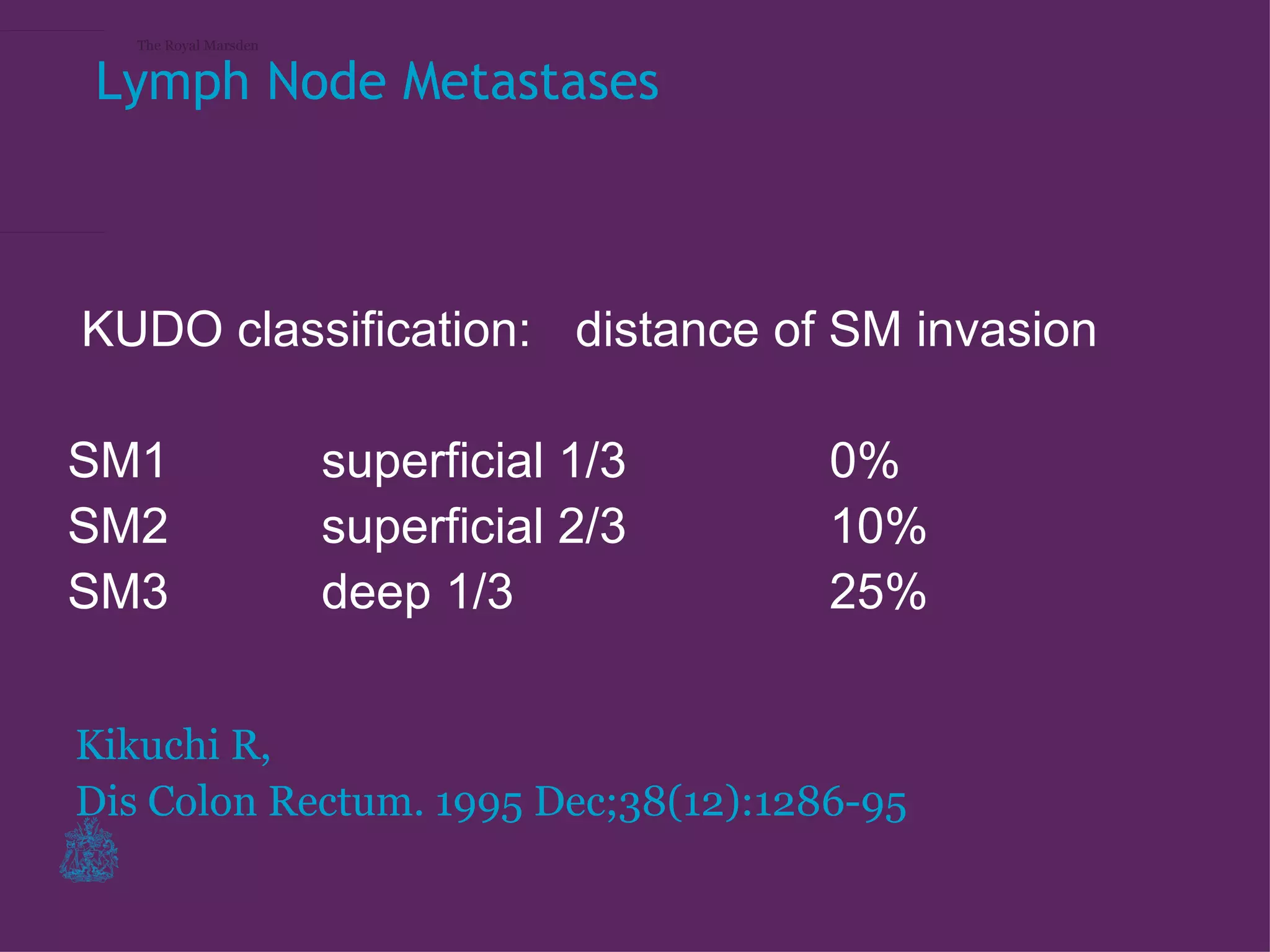
The document discusses staging and treatment of early stage rectal cancer. It provides details on MRI and endoscopic ultrasound for detecting early tumors, especially submucosal invasive tumors. It notes that MRI staging of early polyps can identify T1 or T2 tumors and guide decisions on local excision or total mesorectal excision surgery. The conclusion emphasizes that MRI is useful for evaluating and monitoring early stage rectal tumors, and helps determine appropriate treatment such as local excision or surgery.