Downloaded 852 times





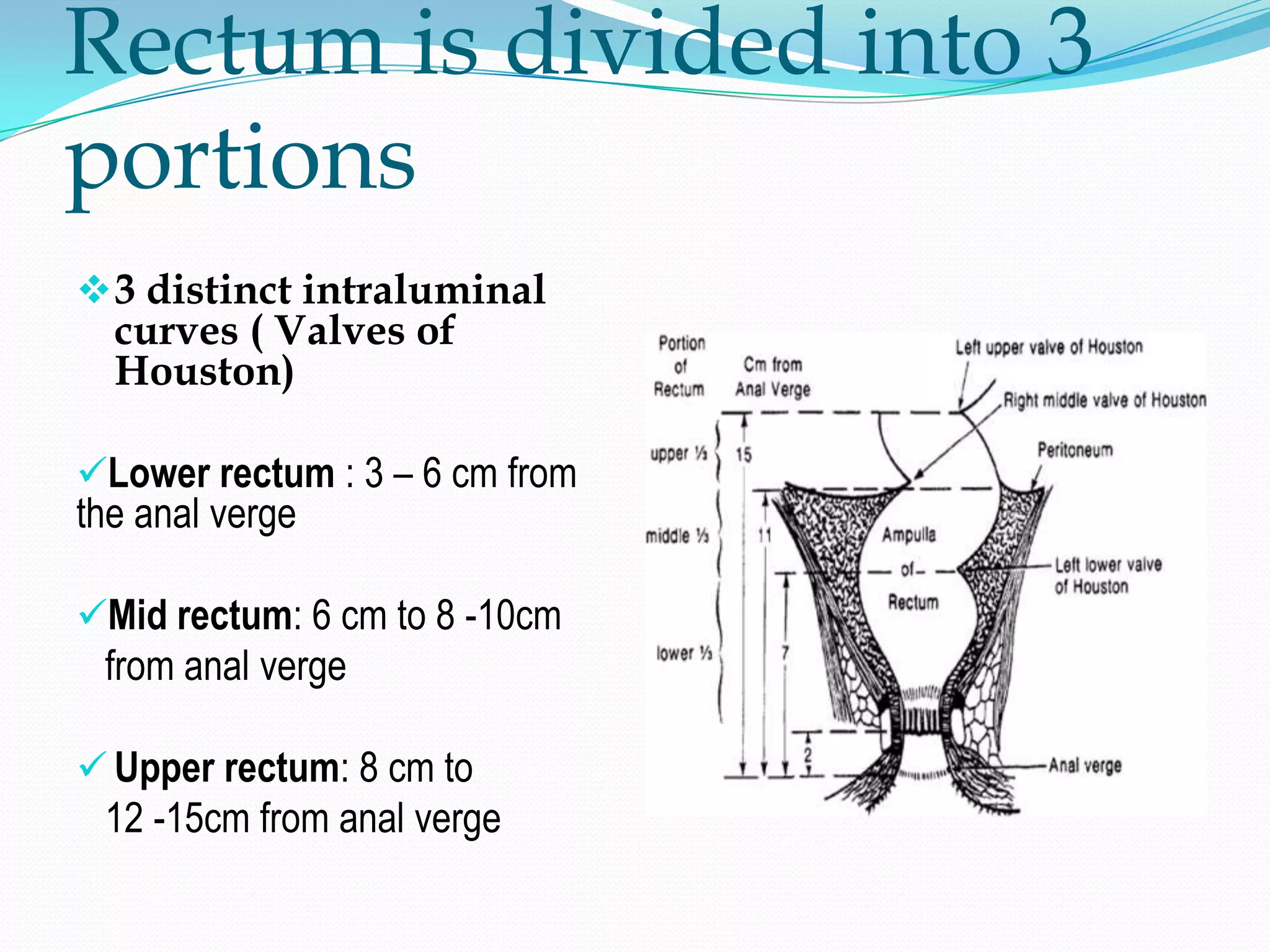




















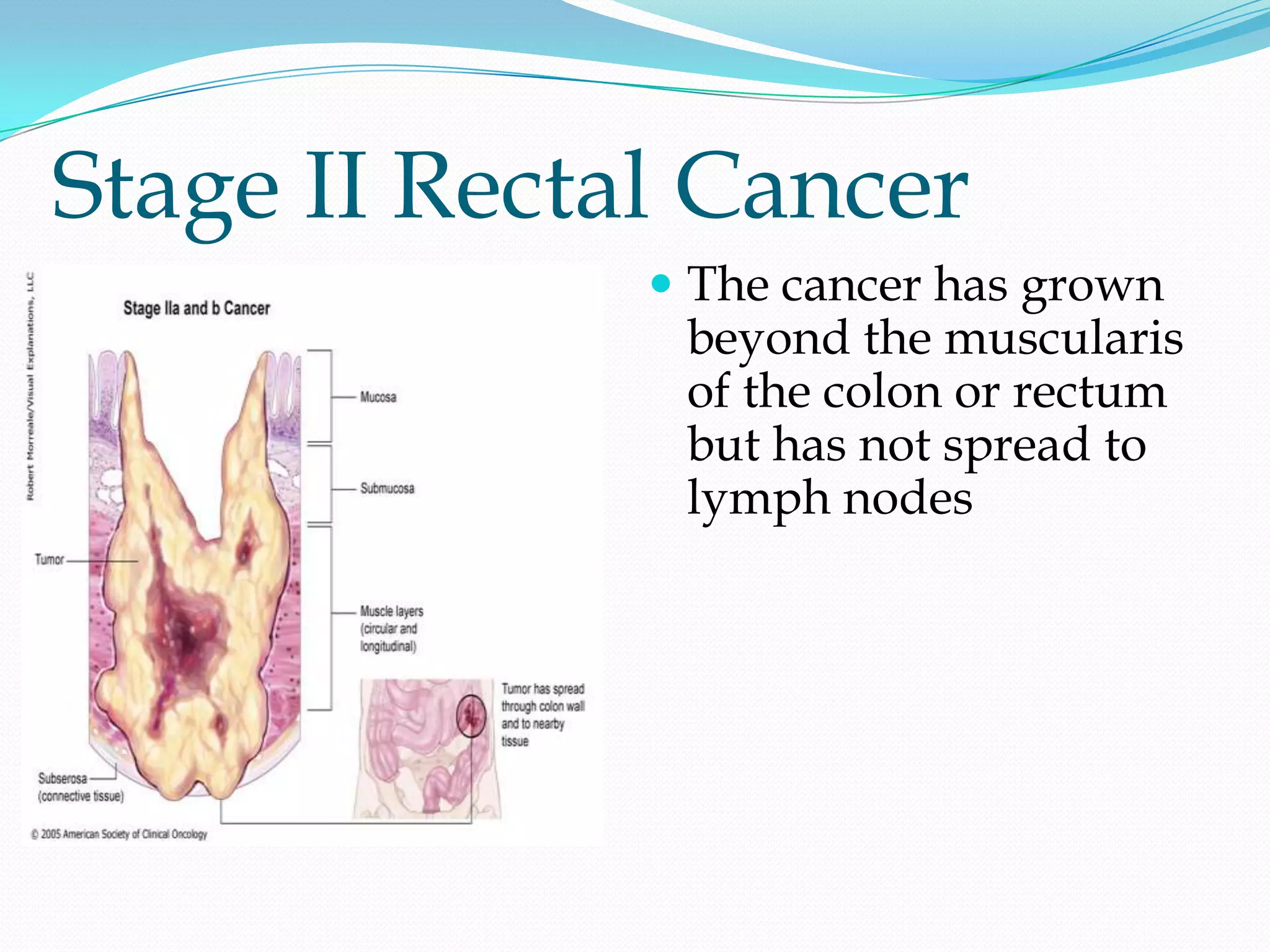

























































































This document provides information on colorectal cancer epidemiology, anatomy, staging, diagnosis and treatment. It discusses: - Colorectal cancer is the 3rd most common cancer in the US, with over 100,000 new cases annually and a lifetime risk of 1 in 10 for men and 1 in 14 for women. - The rectum is located in the pelvis and is divided into lower, mid, and upper portions. It has various blood, nerve and lymphatic supplies. - Staging involves determining the depth of invasion (T stage), lymph node involvement (N stage), and presence of metastases (M stage). Treatment involves surgery with the aim of local control and survival while preserving function












































































