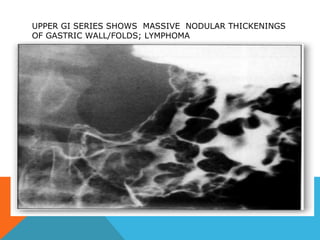
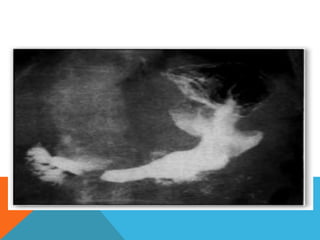
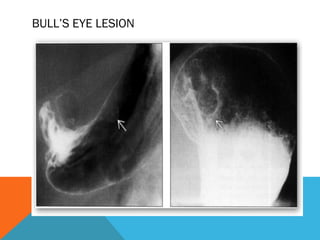
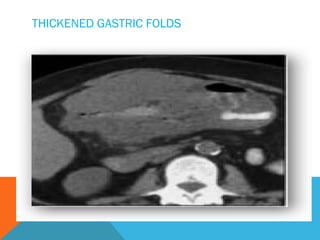
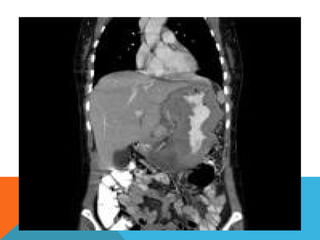
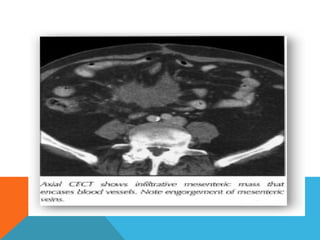
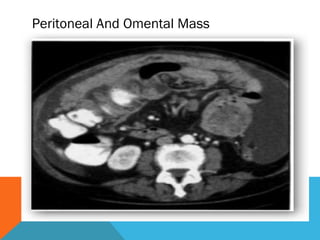
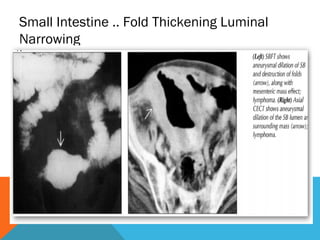
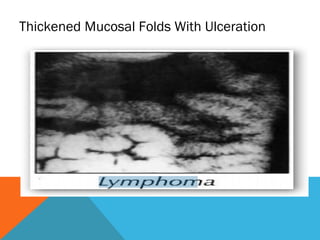
Radiology plays an important role in evaluating gastrointestinal lymphoma. Primary gastrointestinal lymphoma arises in the lymphatic tissue of the bowel rather than lymph nodes. Common sites of involvement include the stomach, small bowel, and colon. On imaging, gastrointestinal lymphoma can appear as thickened folds, masses, strictures, or diffuse bowel wall thickening. Staging involves assessing for involvement of lymph nodes, adjacent organs, or distant metastases. Radiology is useful for diagnosis, evaluating extent of disease, and monitoring treatment response in gastrointestinal lymphoma.