Downloaded 48 times















































![Level Vc – Lateral supraclavicular
NEW LEVEL
• From Transverse cervical vessels cranially to 2 cm above the sternoclavicular joint.
• Its contour stops at same level of IV a (lower jugular) [NOT MEDIAL SUPRACLAVICULAR – LEVEL IV b]
• Corresponds to “Supraclavicular fossa” aka Triangle of Ho (N3b definition of Ca Npx)
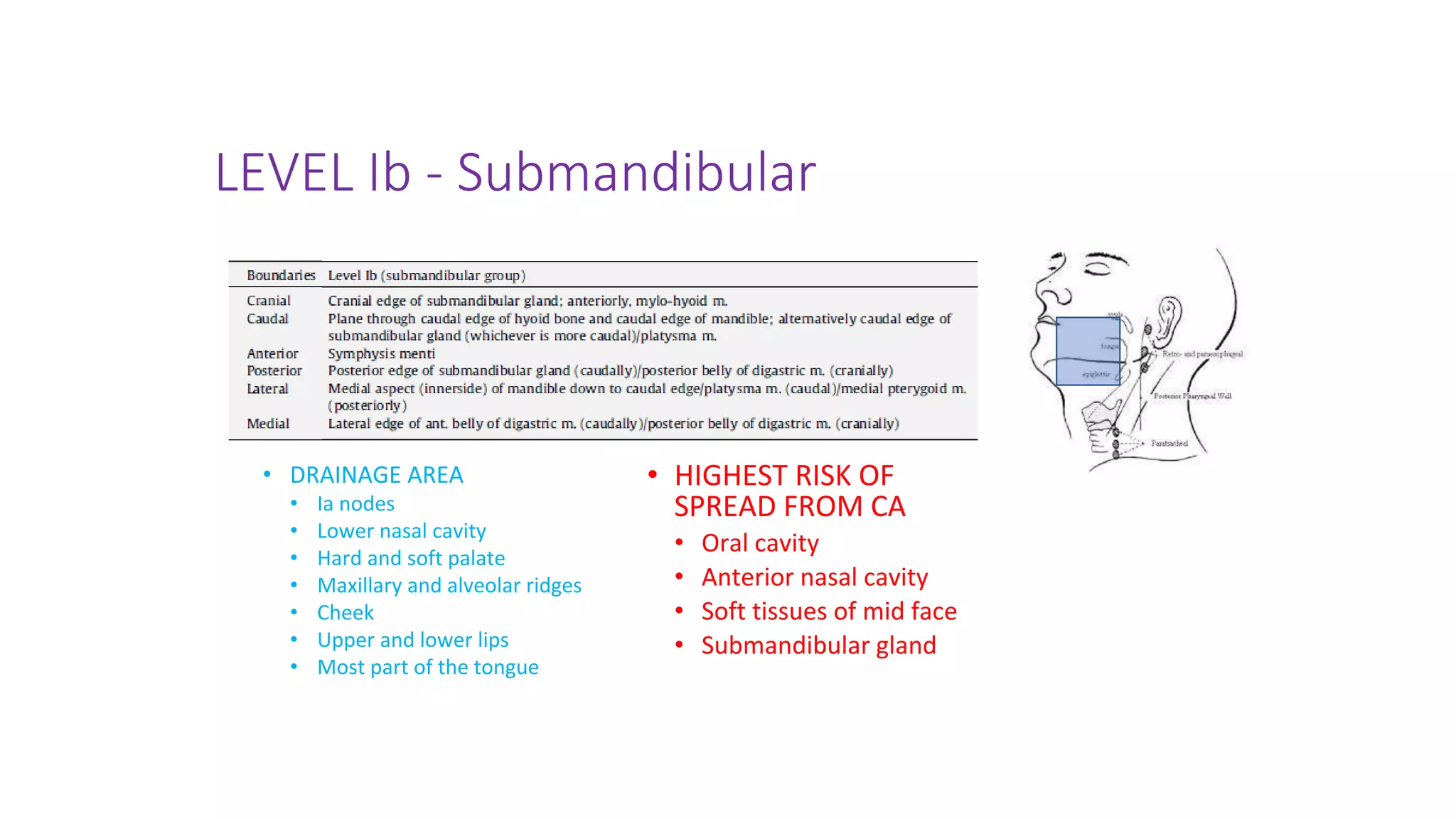
• DRAINAGE AREA
• Posterior triangle nodes
– Level Va and Vb
• HIGHEST RISK OF SPREAD
FROM CA
• Nasopharynx](https://image.slidesharecdn.com/canpxcontouring-220827143943-1e09b6f4/75/Ca-Nasopharynx-contouring-pptx-54-2048.jpg)













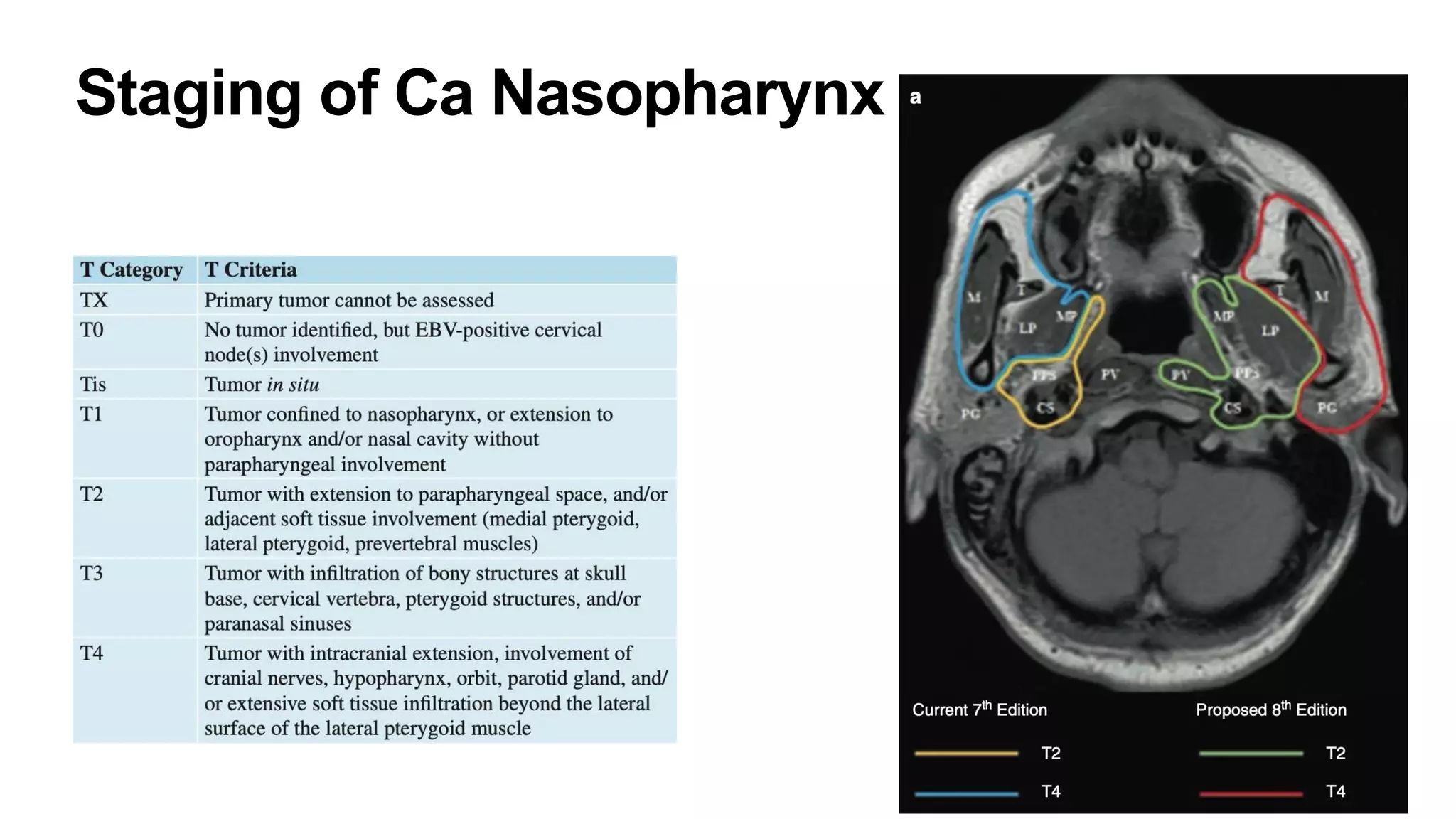
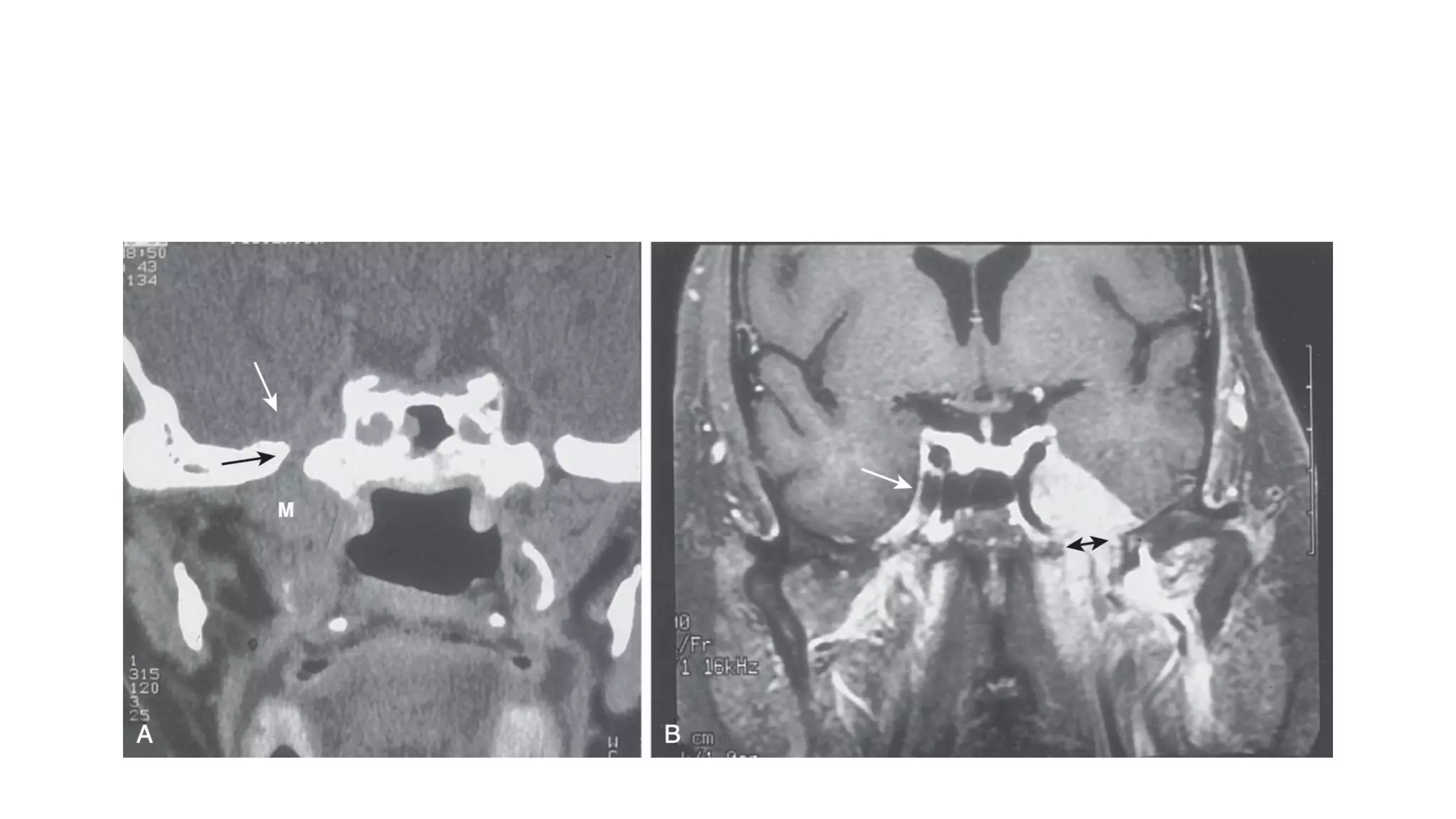
This document provides guidance on contouring for nasopharyngeal carcinoma (NPC) radiation treatment planning. It discusses the anatomy and patterns of spread of NPC, as well as staging. It describes how to delineate the primary gross tumor volume (GTVp), clinical target volumes (CTVs) including high-risk (CTVp1) and intermediate-risk (CTVp2) volumes. It also covers nodal CTV delineation (CTVn1, CTVn2, CTVn3) and discusses lymph node levels and risk of spread. Margins around critical organs and intracranial extension guidelines are also summarized. The document aims to provide a comprehensive overview of target volume delineation for NPC