Downloaded 90 times

































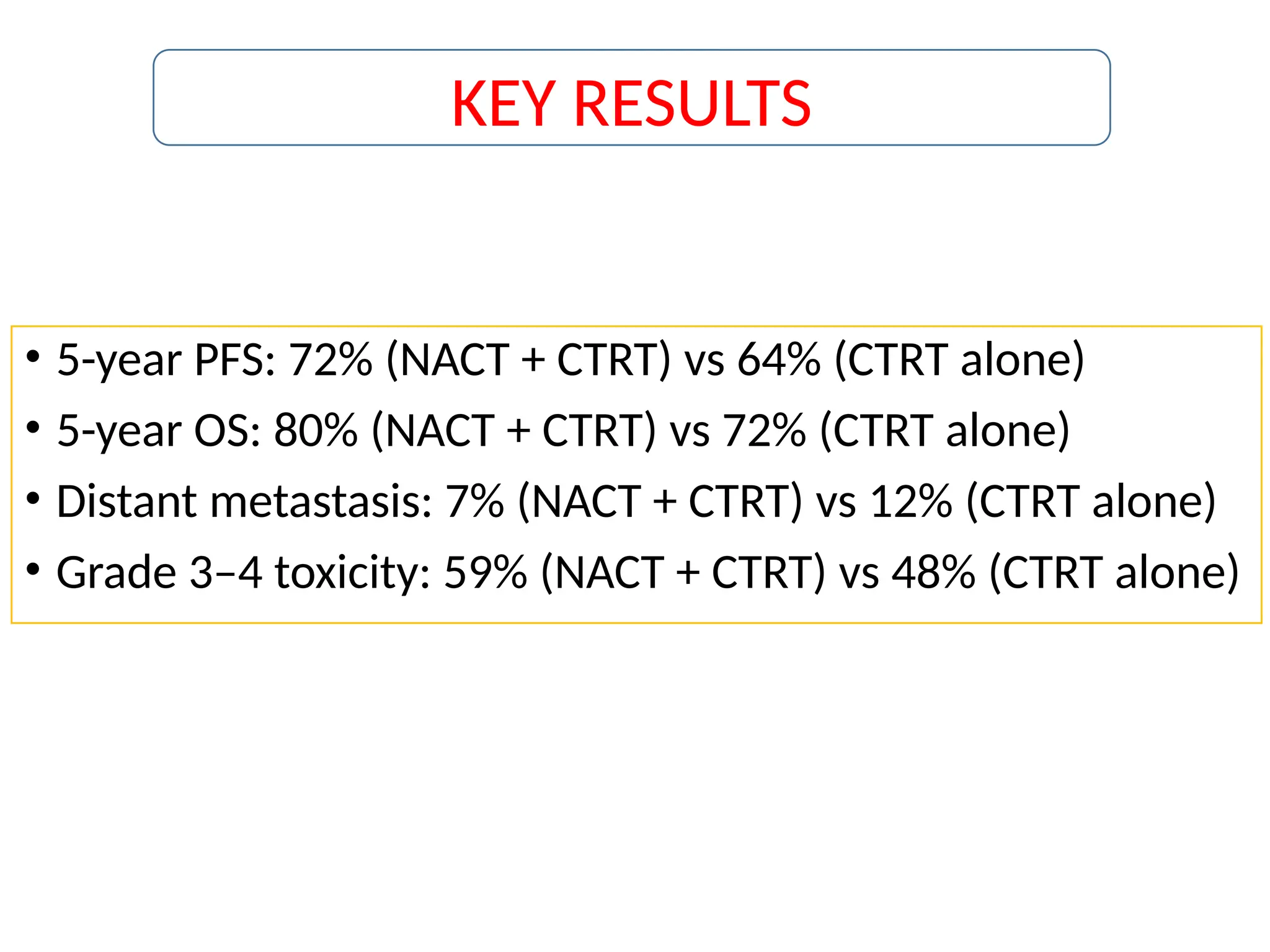

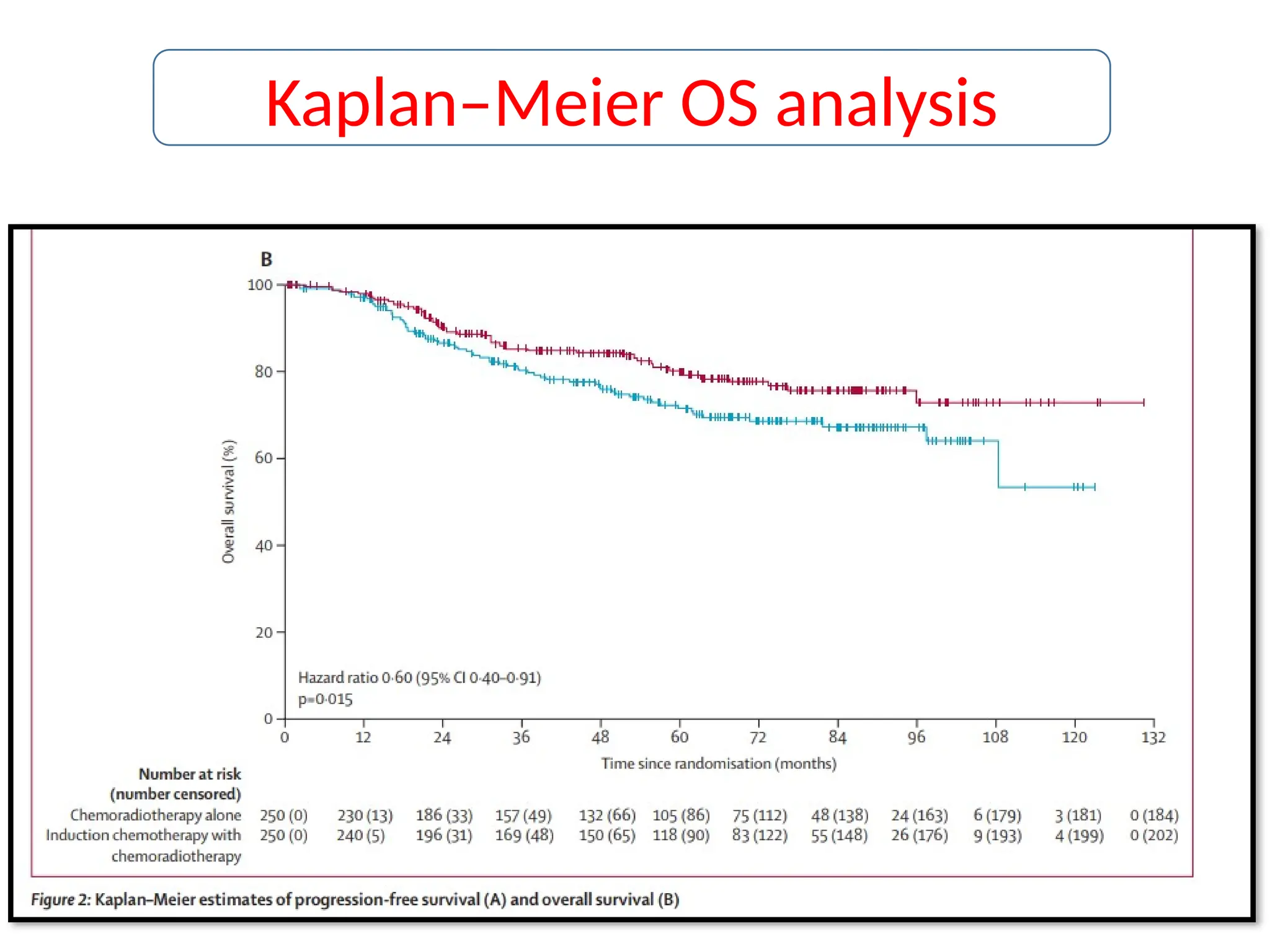














The Interlace trial studied the effect of adding induction chemotherapy to standard chemoradiotherapy in patients with locally advanced cervical cancer, involving 500 participants across 32 medical centers globally. Results indicated improved progression-free survival (72% vs. 64%) and overall survival (80% vs. 72%) in the combined treatment arm, although there was increased toxicity associated with induction chemotherapy. Overall, the findings suggest that the combination of induction chemotherapy followed by chemoradiotherapy may become a new standard of care for this patient group.








































![management of advanced cervical cancer [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/managementofadvancedcervicalcancerautosaved-230926014710-62f747b3-thumbnail.jpg?width=640&height=640&fit=bounds)













































