This document discusses esophageal cancer. Some key points:
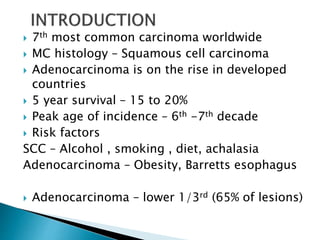
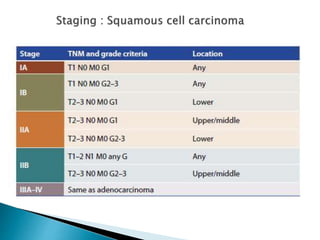
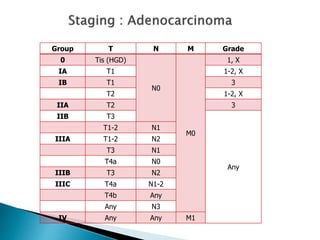
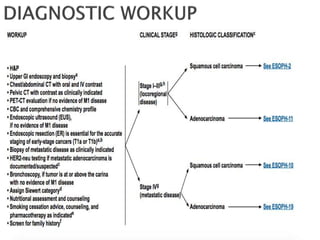
- Squamous cell carcinoma and adenocarcinoma are the most common histologies. Risk factors include smoking, alcohol, obesity, and Barrett's esophagus.
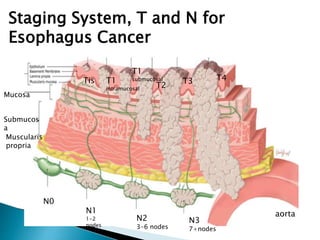
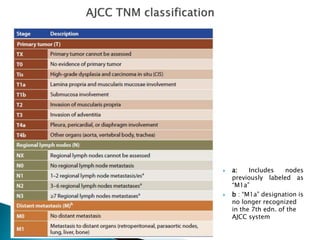
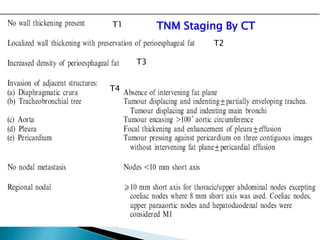
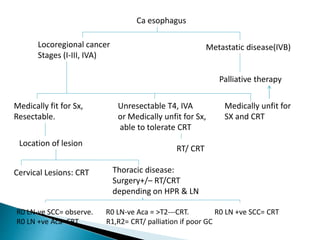
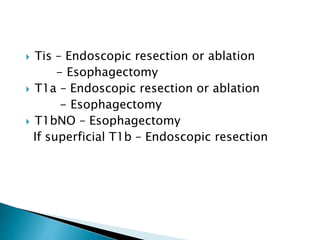
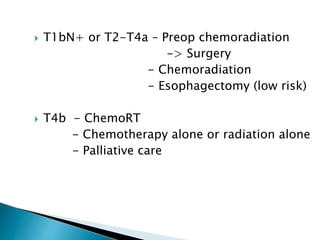
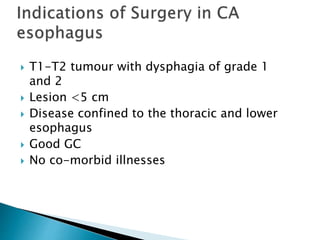
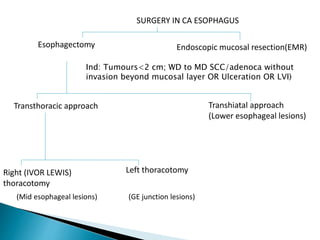
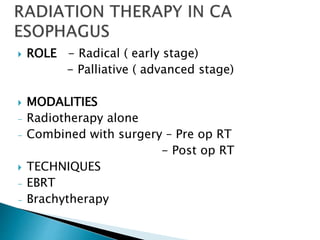
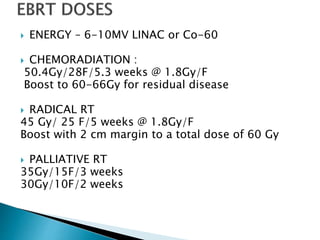
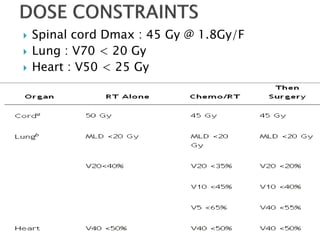
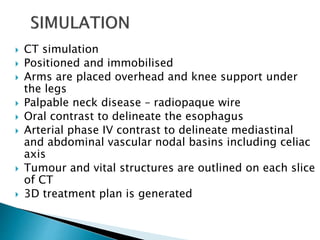
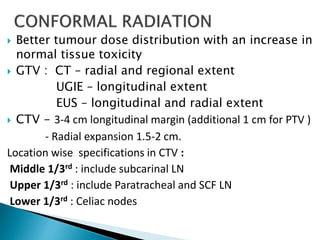
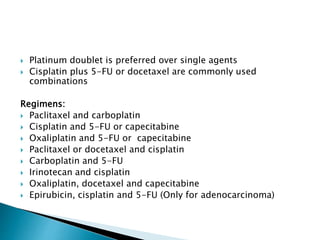
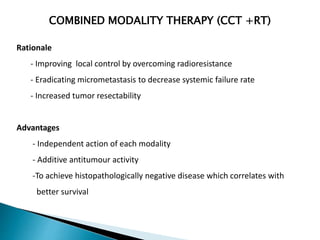
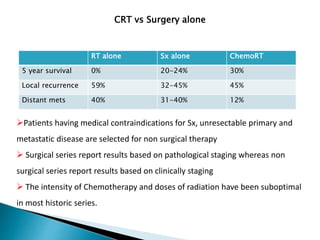
- Staging uses the TNM system. Treatment depends on stage but may include surgery, chemotherapy, radiation therapy, or a combination.
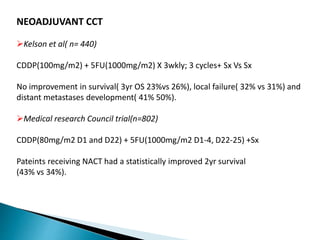
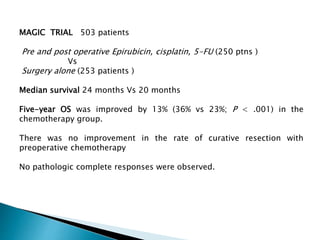
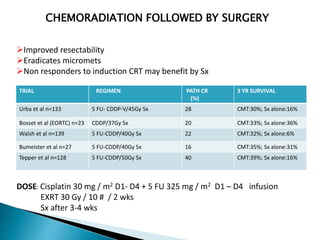
- For locally advanced stages, neoadjuvant chemoradiation can improve resectability and survival compared to surgery alone. The MAGIC trial showed improved survival with perioperative chemotherapy compared to surgery alone.
- Prognosis remains poor with 5-year survival rates of 15-20%, though outcomes have improved with multimod











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




