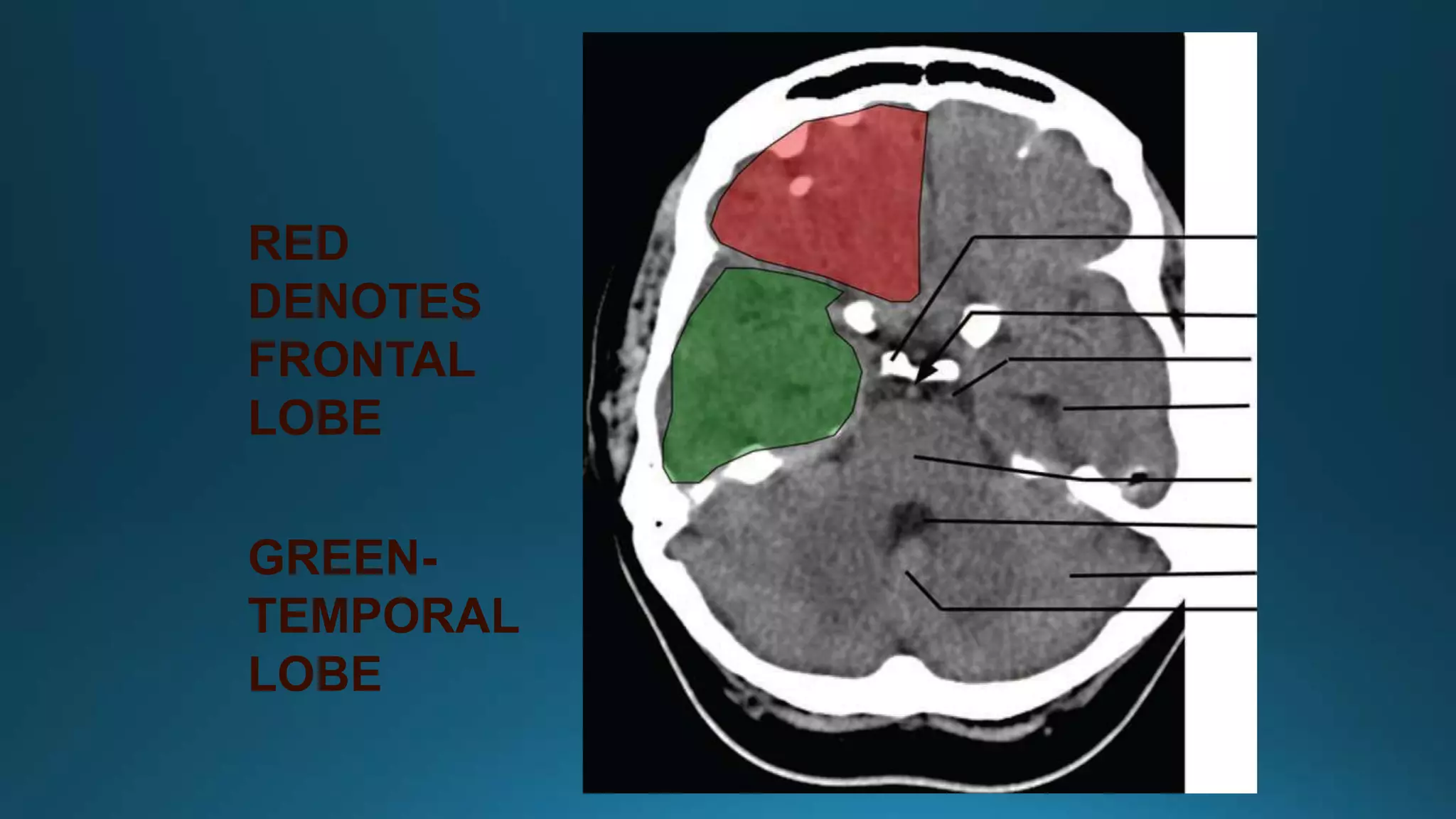
This document provides information about brain anatomy and stroke imaging. It describes the major lobes of the brain including the frontal, temporal, parietal and occipital lobes. It then discusses stroke, noting the differences between ischemic and hemorrhagic stroke. Imaging goals for acute stroke are outlined, focusing on distinguishing between ischemic stroke and hemorrhage, and identifying patients who may benefit from reperfusion therapies. Various MRI sequences are described for imaging acute and chronic strokes at different time points.