Learning objectives
• Listthe systemic effects of inflammation
• Discuss the regulation of inflammation
• Discuss factors responsible for the variation in inflammatory response
• Identify the different morphologic patterns of non-suppurative inflammation
• Illustrate the fate of the different morphologic patterns of non-suppurative
inflammation
• Define suupurative inflammation
• Classify suppurative inflammation
3.
Systemic effects
•Fever, malaise,loss of appetite: Cytokines interleukin-l (IL-1) and tumor
necrosis factor (TNF) secreted by leukocytes in are involved in the
pathogenesis of fever
•Leukocytosis : increased number of leucocytes >12000/cmm
•Changes in plasma protein levels: increase in acute phase reactants as C-
reactive protein, elaboration of certain cytokines (IL-1, IL-6) and elevation
of ESR (erythrocyte sedimentation rate)
5.
• Shock mayoccur in severe cases. Massive release of cytokine TNF-a, a
mediator of inflammation, in response to severe tissue injury or infection
results in profuse systemic vasodilatation, increased vascular permeability
And intravascular volume loss. The net effect of these changes is
hypotension and shock.
6.
REGULATION OF INFLAMMATION
•Normally, inflammation is kept in check by the inbuilt regulatory system to
resolve its harmful effects.
• Acute phase reactants A variety of acute phase reactant (APR) proteins are
released in plasma in response to tissue trauma and infection. Their major
role is to protect the normal cells from harmful effects of toxic molecules
generated in inflammation and to clear away the waste material.
• APRs include the following:
7.
• Certain cellularprotection factors (e.g. a1-antitrypsin)
• Some coagulation proteins (e.g. fibrinogen, plasminogen)
• Transport proteins (e.g. ceruloplasmin)
• Immune agents (e.g. serum amyloid A)
• Stress proteins (e.g. heat shock proteins)
• Antioxidants
8.
• Glucosteroids Theendogenous glucocorticoids act as anti-inflammatory
agents.
• Anti-inflammatory chemical mediators: PGE2 or prostacyclin have both
pro-inflammatory as well as anti-inflammatory actions.
9.
FACTORS DETERMINING VARIATIONIN
INFLAMMATORY RESPONSE
• Factors Involving the Organisms
• i) Type of injury and infection For example, skin reacts to herpes simplex
infection by formation of vesicle and to streptococcal infection by formation of
boil; lung reacts to pneumococci by occurrence of lobar pneumonia while to
tubercle bacilli it reacts by granulomatous inflammation.
• ii) Virulence Many species and strains of organisms may have varying virulence
e.g. the three strains of C. diphtheria (gravis, intermedius and mitis) produce the same
diphtheria exotoxin but in different amount.
• iii) Dose The concentration of organism in small doses produces usually local
lesions while larger dose results in more severe spreading infections.
10.
• iv) Portalof entry Some organisms are infective only if administered by
particular route e.g. Vibrio cholerae is not pathogenic if injected
subcutaneously but causes cholera if swallowed.
• v) Product of organisms Some organisms produce enzymes that help in
spread of infections e.g. hyaluronidase by Clostridium welchii, streptokinase by
streptococci, staphylokinase and coagulase by staphylococci.
11.
• Factors Involvingthe Host
• i) Systemic diseases Certain acquired systemic diseases in the host are
associated with impaired inflammatory response liver, chronic alcoholism,
bone marrow suppression from various causes (drugs, radiation, idiopathic).
These conditions render the host more susceptible to infections.
12.
• ii) Immunestatus of host Patients who are immunosuppressed from
congenital or acquired immunodeficiency have lowered inflammatory
response and spread of infections occurs rapidly e.g. in AIDS, congenital
immunodeficiency diseases, diabetes mellitus, protein calorie malnutrition,
starvation.
• iii) Congenital neutrophil defects Congenital defects in neutrophil
structure and functions result in reduced inflammatory response.
13.
• iv) LeukopeniaPatients with low WBC count with neutropenia or
agranulocytosis develop spreading infection.
• v) Site or type of tissue involved For example, the lung has loose texture as
compared to bone and, thus, both tissues react differently to acute
inflammation.
• vi) Local host factors For instance, ischaemia, presence of foreign bodies
and chemicals cause necrosis and thus cause more harm.
14.
MORPHOLOGY OF ACUTE
INFLAMMATION
Afew morphologic varieties of acute inflammation are described below:
• The appearance of escaped plasma determines the morphologic type of
inflammation
• Catarrhal Inflammation:
•It is a mild form of acute
inflammation.
• It occurs in any mucous surface as
nasal passages, bronchi,
gastrointestinal tract, e.g. common cold
and some forms of colitis.
• It manifests itself by excessive mucus
secretion.
17.
• Serous Inflammation:
•It is a mild form
• It is characterized by excessive clear
watery fluid with variable protein
content, but no fibrin
• Affects serous cavities and skin as in
burns (blisters of burn)
18.
3. Serofibrinous andfibrinous inflammation
Moderate form
Characterized by: exudate rich in fibrin
Sites:
serous cavities
joints
lung alveoli
Membranous (Pseudomembranous)
Inflammation:
• Itis characterized by formation of a false membrane on the mucous
surface e.g. diphtheria, bacillary dysentery.
• Pathogenesis: bacteria remain on the mucosal surface and produce
powerful exotoxins which cause patchy mucosal necrosis and acute
inflammation of the submucosa. As a result of denudation of epithelium,
plasma exudes on the surface where it coagulates, and together with necrotic
epithelium, forms false membrane that gives this type of inflammation its
name.
21.
Severe form
Characterized by:formation of superficial dull opaque yellow membrane
which when pealed leave bleeding surface
Sites: mucus surfaces
Examples:
diphtheria
bacillary dysentry
5. Allergic inflammation
Mildto severe
It is due to hypersensitivity reaction
which causes tissue injury
Characterized by: exudate rich in
eosinophils
Purulent or suppurativeinflammation
• This type of inflammation is caused by pyogenic (pus-forming) bacteria e.g.
staphylococcus, streptococcus hemolyticus or gonococcus. It is characterized
by suppuration (pus formation).
26.
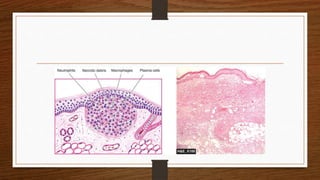
Pus
• It isa purulent inflammatory exudate, consisting of living and dead bacteria
and their toxins, necrotic cells, living neutrophils, dead neutrophils (pus cells),
macrophages and some times red cells.
• Characters: It appears as a thick, turbid, yellow, odorless alkaline fluid. It
does not clot on standing because its fibrinogen content is destroyed by the
proteolytic enzymes.
28.
Pathogenesis (Mechanism ofpus formation):
• The pyogenic microorganisms cause:
• Excessive tissue destruction (necrosis) by its toxins.
• Chemotactic effect on neutrophils.
• Neutrophils killed during their battle with the bacteria form pus cells.
• Pus cells release proteolytic enzymes leading to rapid liquefaction of the
necrotic tissue forming pus. The resulting fluid material mixes with other
inflammatory products (cells & exudate) to form pus.
29.
Classification of suppurativeinflammation
1. Localized suppuration:
Abscess
Boil (furuncle)
Stye
Carbuncle
2. Diffuse suppuration
Phlegmonous inflammation
diffuse suppuration in a body cavity
collection of pus in a lumen pf organ
cellutlitis
30.
Abscess
• Definition: localizedarea of suppuration, characterized by cavity formation
full of pus.
• Cause: the causative organism is commonly staphylococcus aureus which
releases coagulase enzyme leading to localization of infection.
34.
• An abscessmay be discharged to
the surface due to increased
pressure inside or may require
drainage by the surgeon. Due to
tissue destruction, resolution does
not occur but instead healing by
fibrous scarring takes place.
35.
• Special typesof abscesses:
• Boil (furuncle): is a small abscess
related to hair follicles or sebaceous
glands. It is commonly found in the
face, back, neck and in the axilla.
• Stye: is an abscess in the eyelid
related to the eye lashes.
36.
• Carbuncle: isa multilocular
abscess in the skin and
subcutaneous tissue discharging pus
through numerous openings. It is
usually found in the back of the
neck especially in diabetic persons.
Copy protected with Online-PDF-No-Copy.com






















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





