Downloaded 82 times


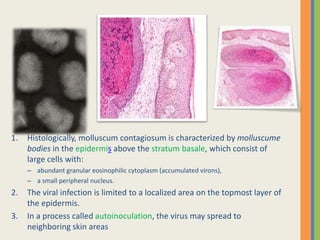







Molluscum contagiosum (MC) is a viral skin infection caused by the molluscum contagiosum virus, affecting primarily children, sexually active adults, and immunocompromised individuals. The virus spreads through skin-to-skin contact and can cause flesh-colored, dome-shaped papules that may last up to 18 months if untreated, with various treatment options available ranging from cryotherapy to antiviral therapies. Although treatment is often unnecessary as lesions can resolve on their own, it may be sought for comfort, cosmetic reasons, and to prevent further spread or complications.
































































































