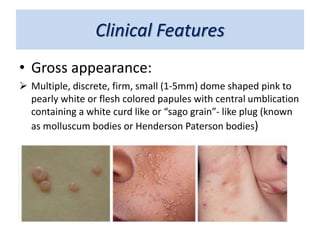
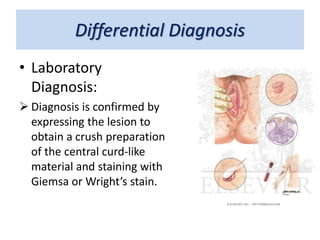
This document discusses molluscum contagiosum, a common viral skin infection caused by the molluscum contagiosum virus. It primarily affects children and sexually active adults. The infection causes multiple pink or white dome-shaped papules with a central umbilication containing a white plug. Lesions are usually found on the trunk, face, extremities and intertriginous areas in children, and the peri-anal and genital areas in adults. While self-limiting, treatment options include surgical removal or destruction of lesions through curettage, electrodessication or cryosurgery, or applying medical treatments like trichloracetic acid or lactic/salicylic acid solutions.




![1.1.2. viral infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-2-viralinfectionsofskincompatibilitymode-120714004456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)











![Fungal infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/fungalinfectionsofskincompatibilitymode-130321223403-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















































