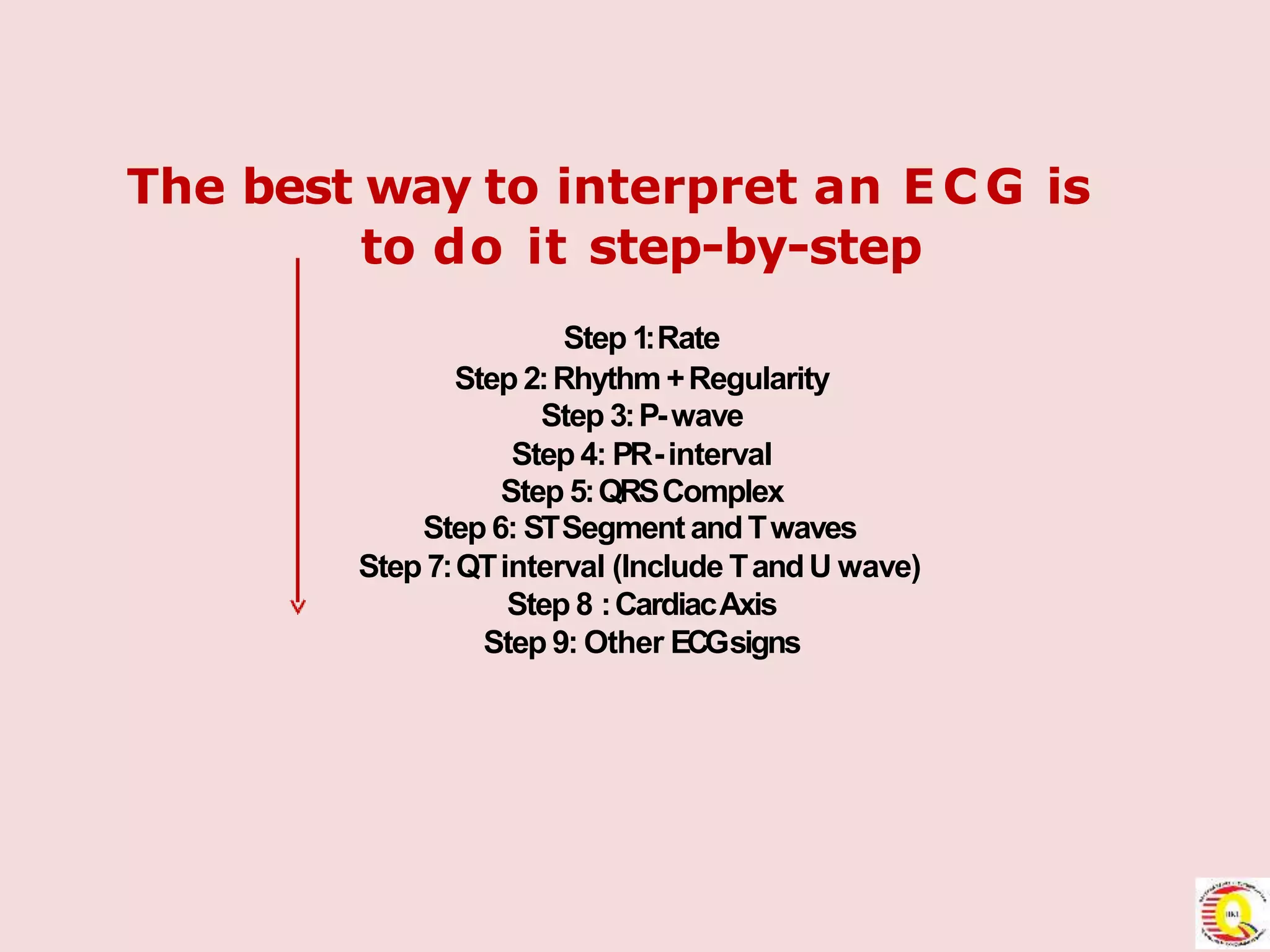
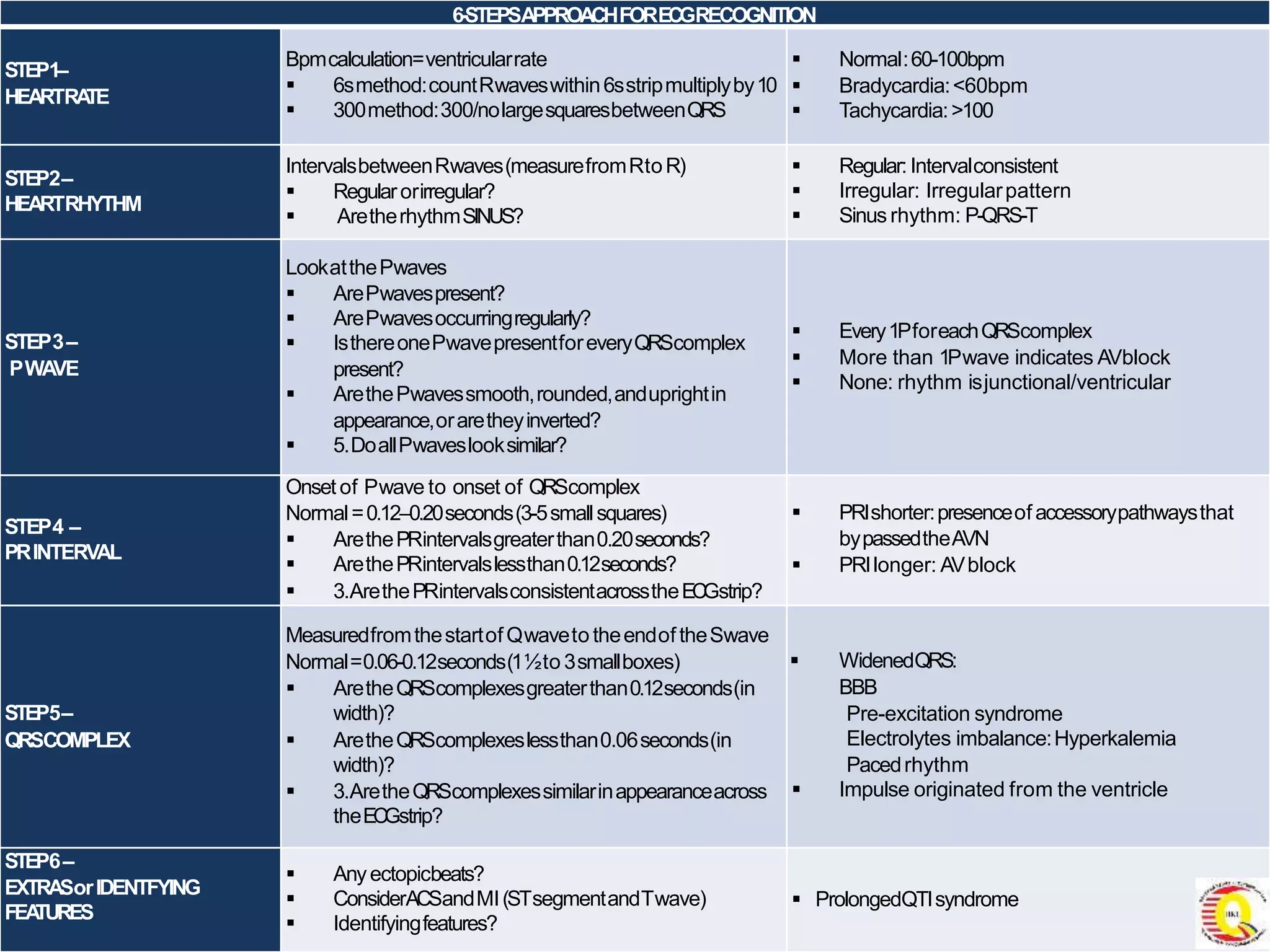
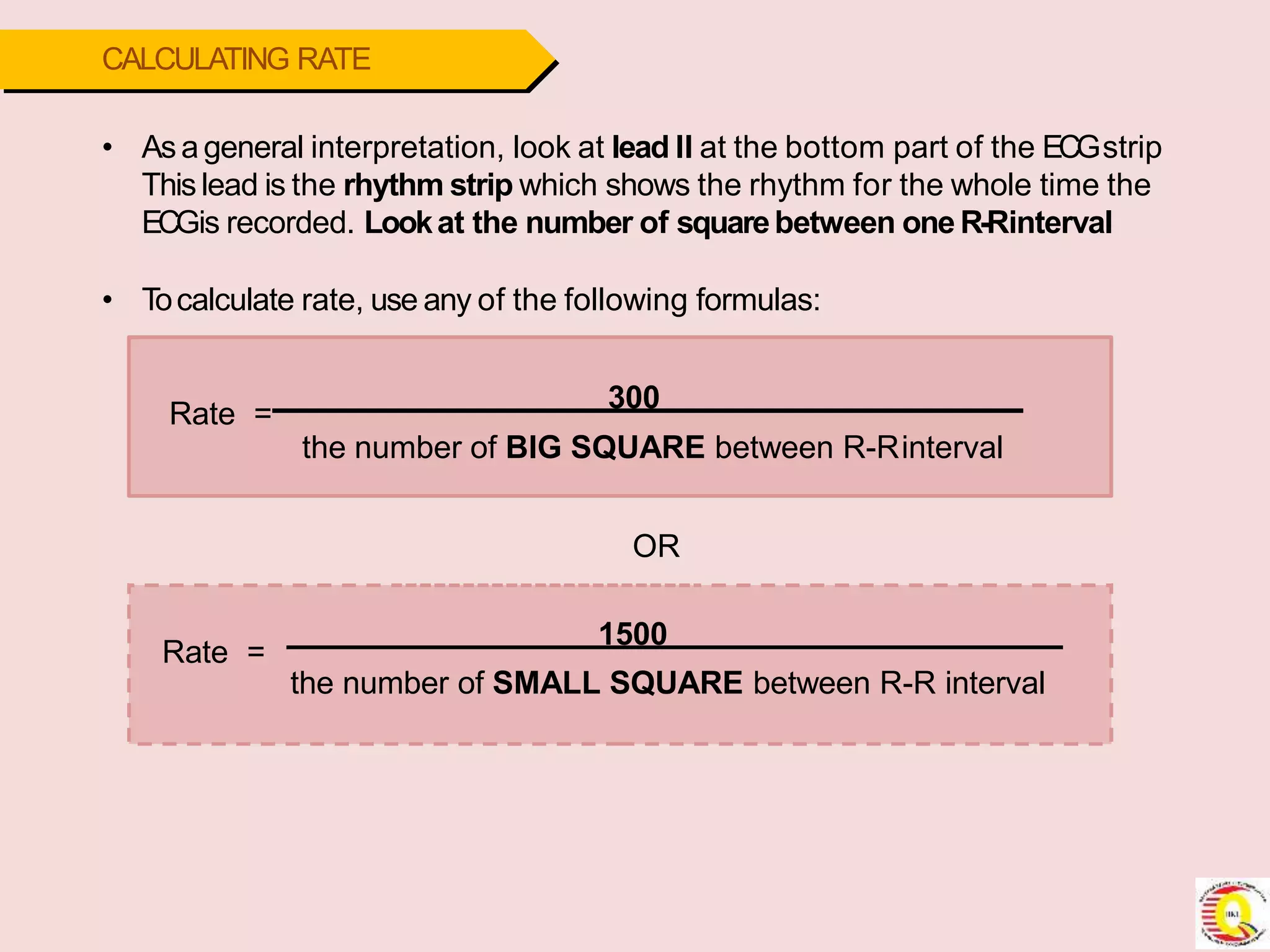
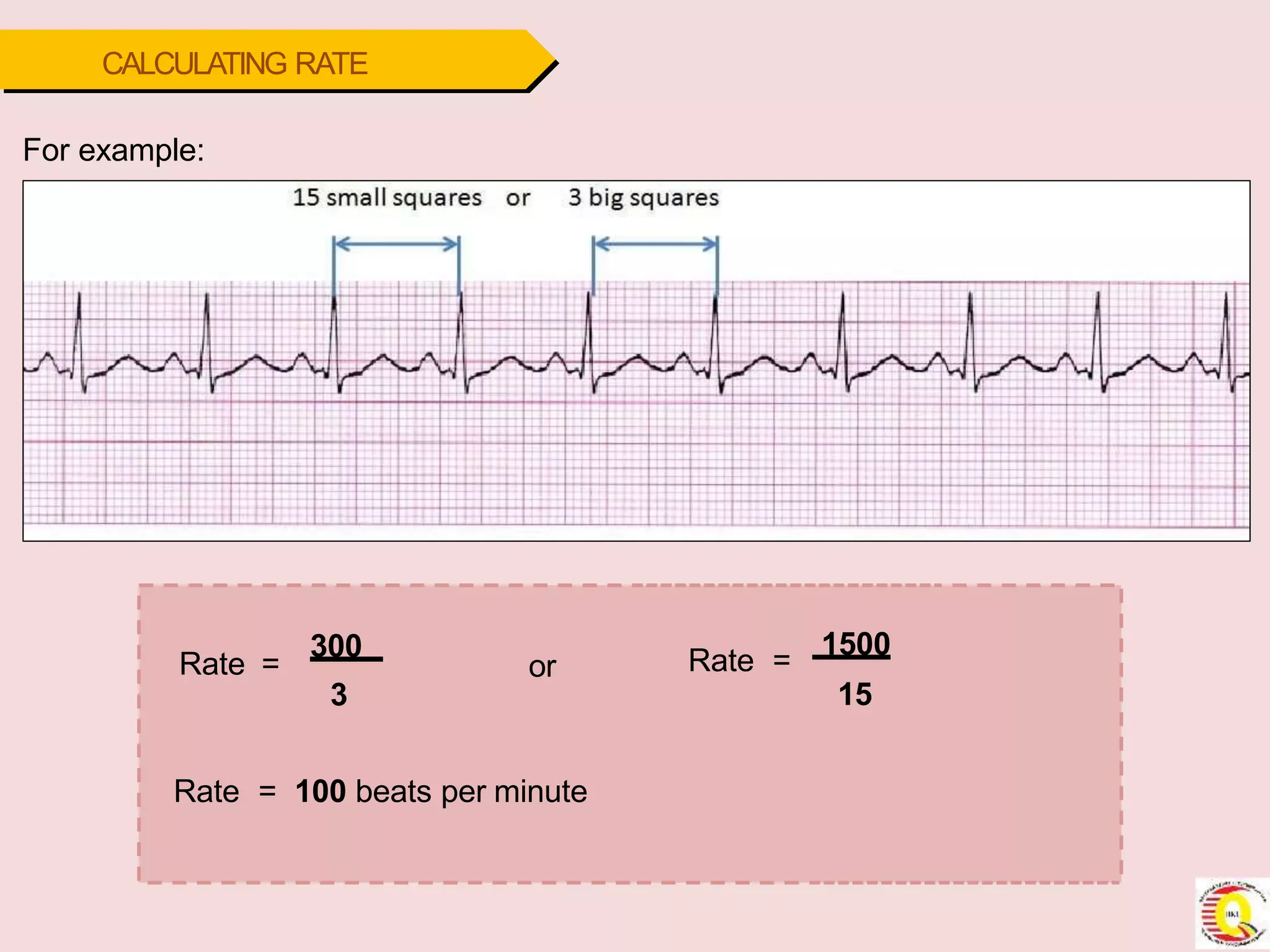
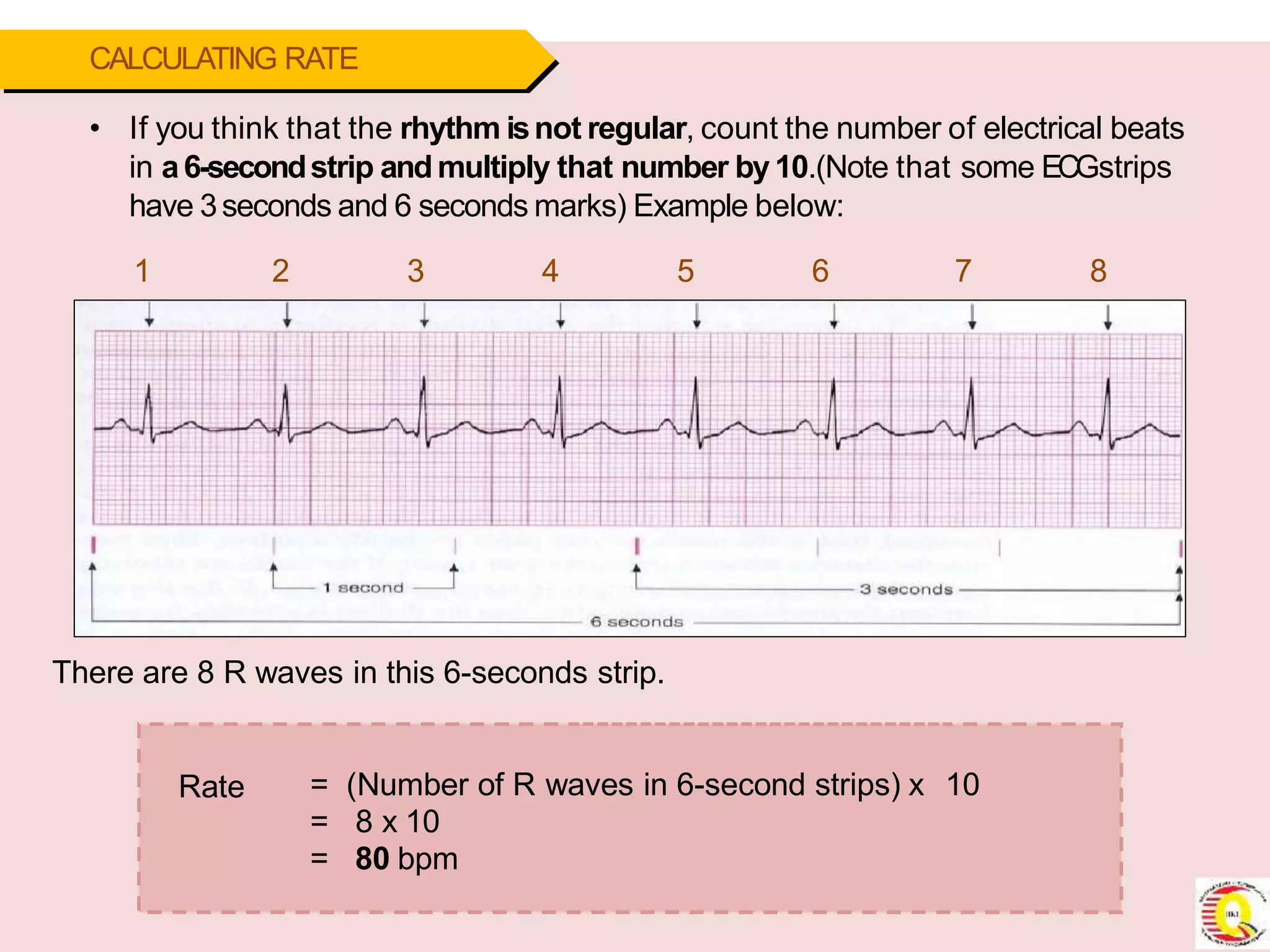
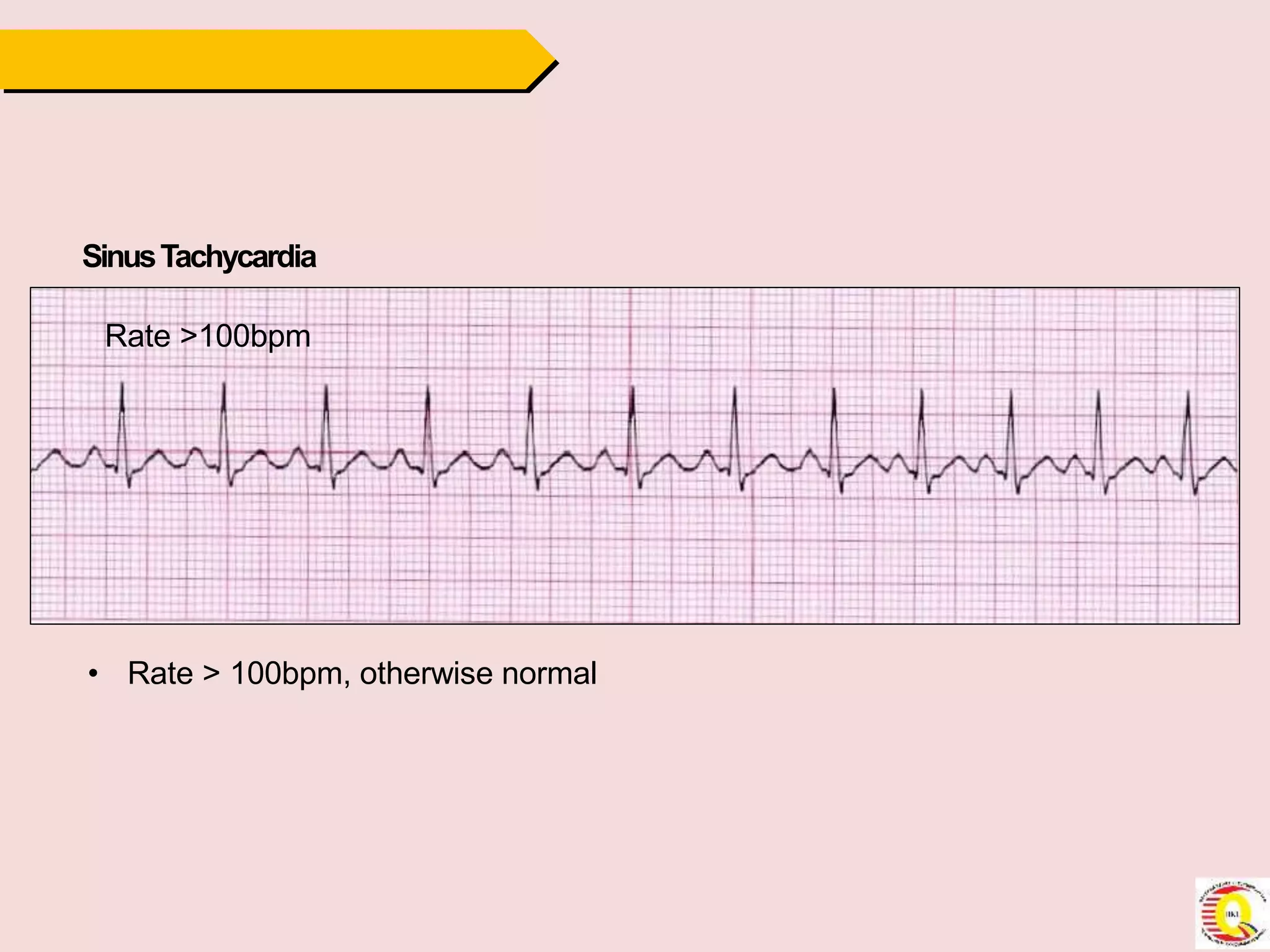
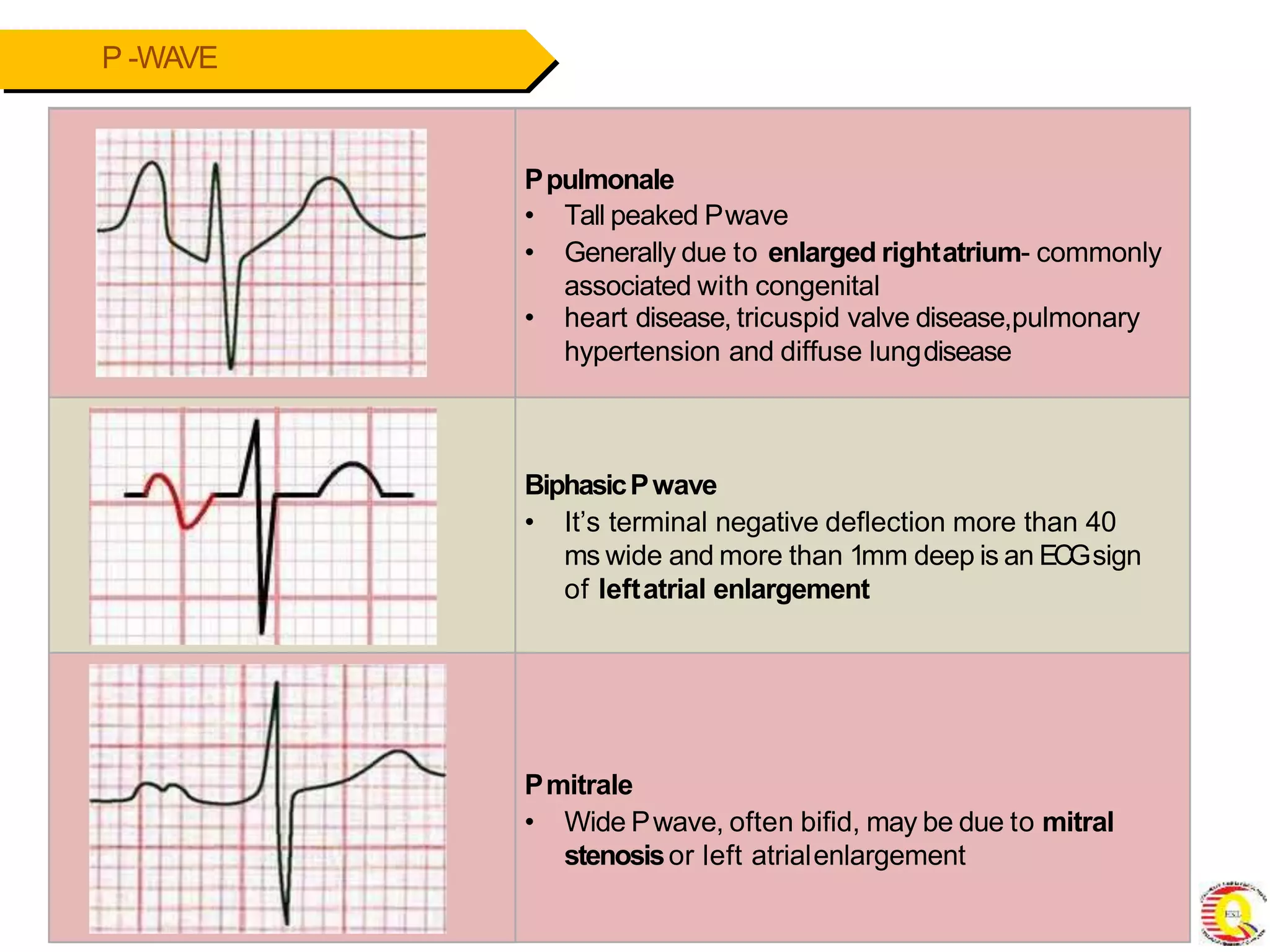
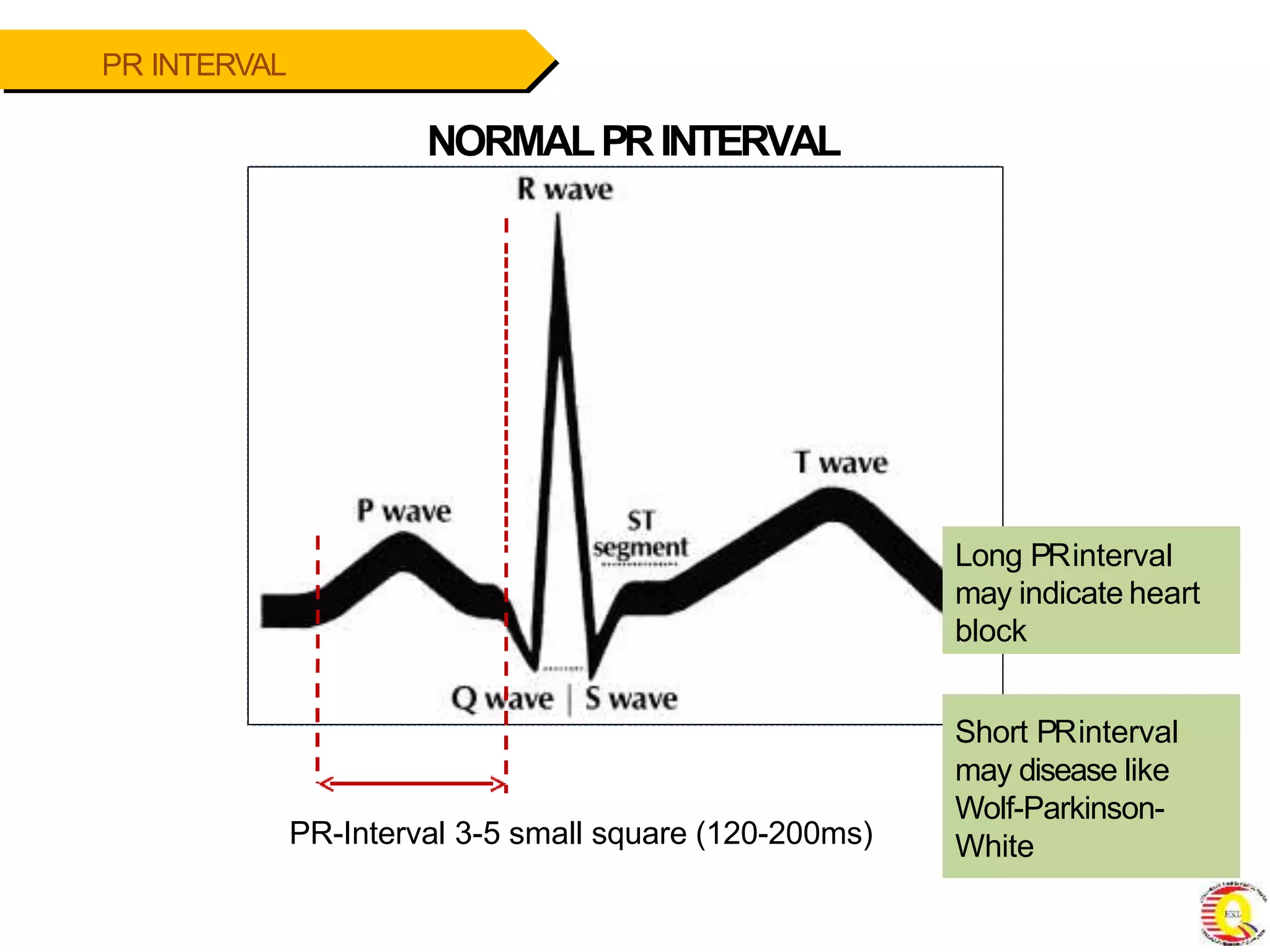
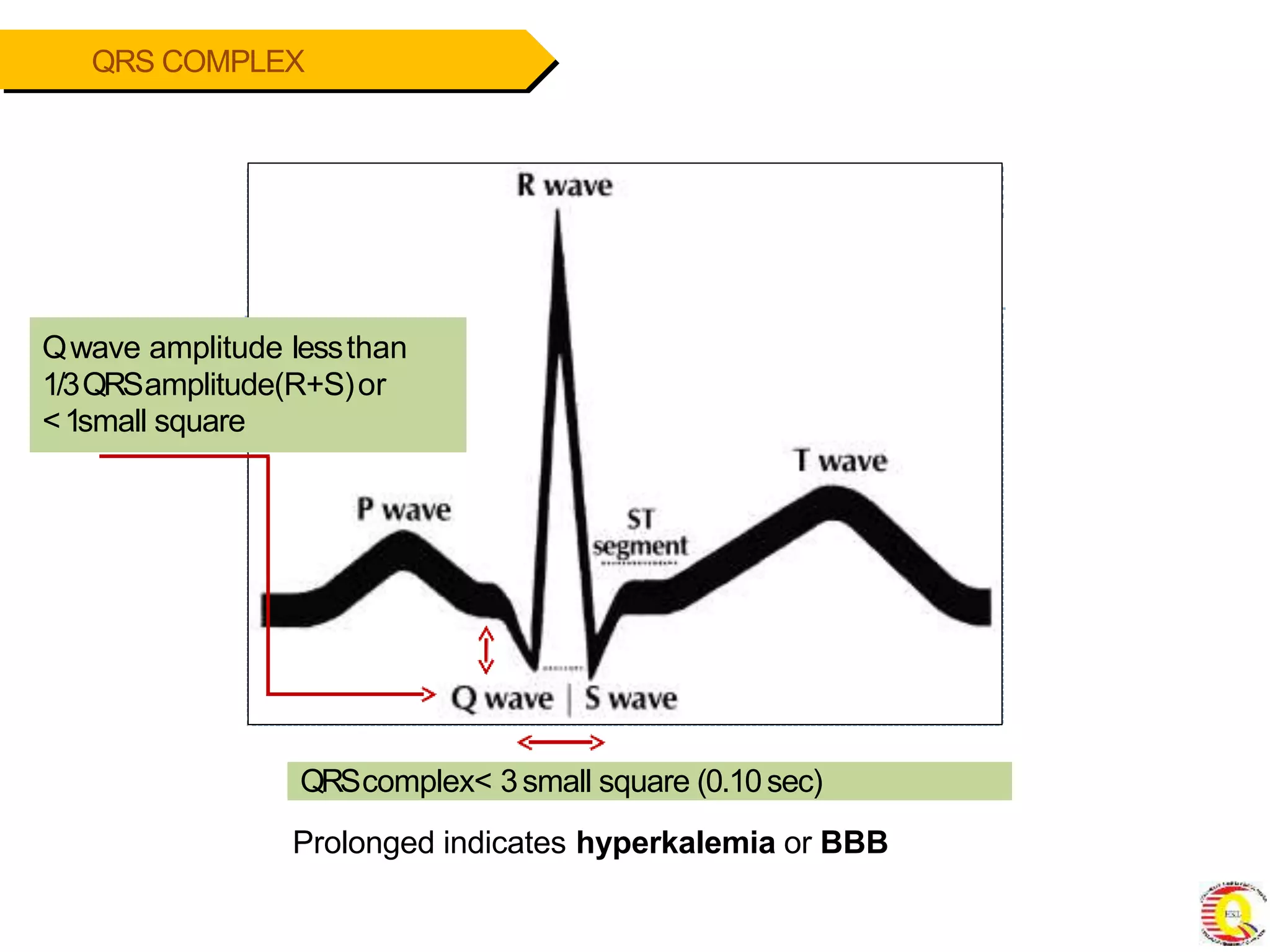
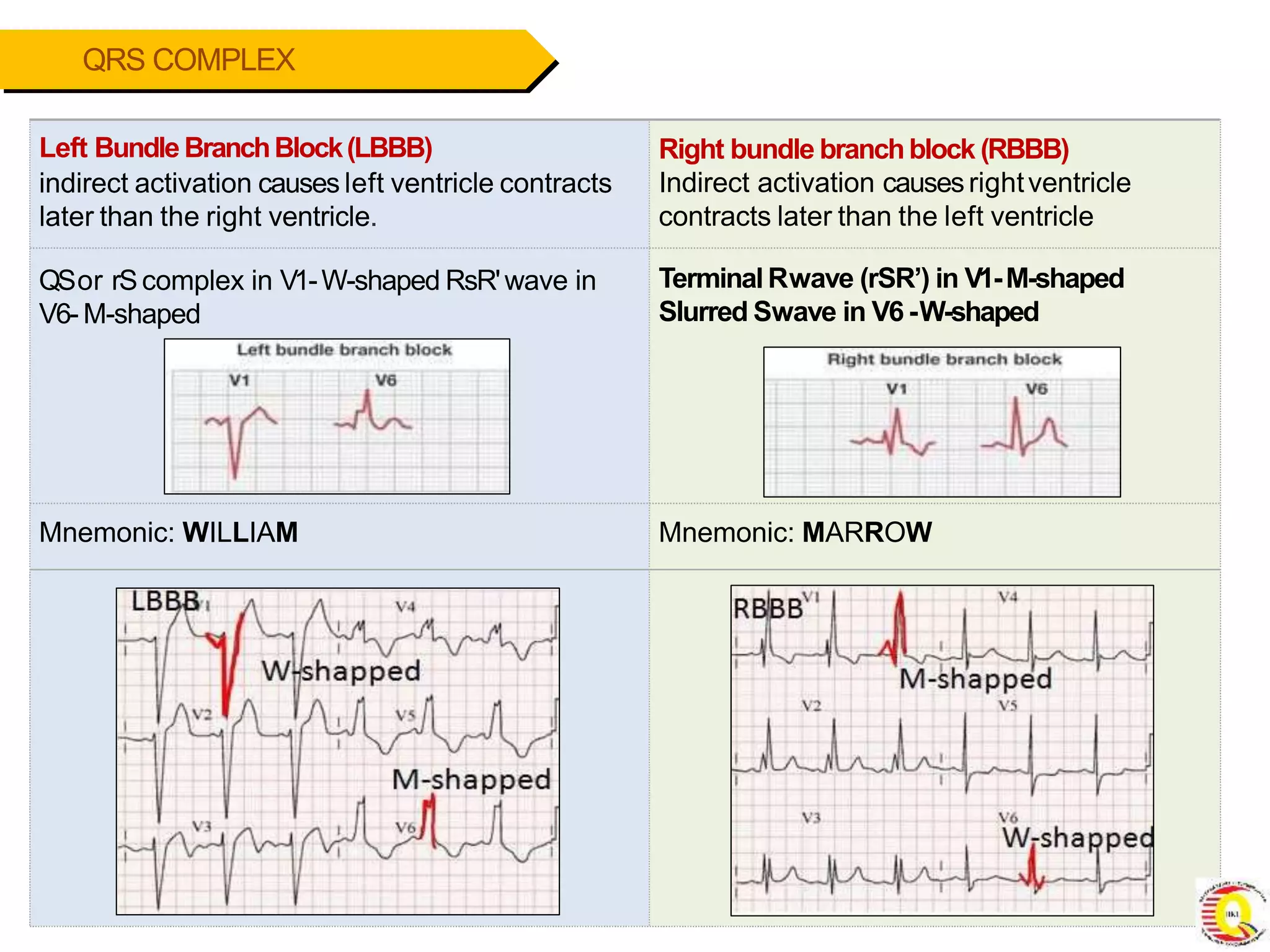
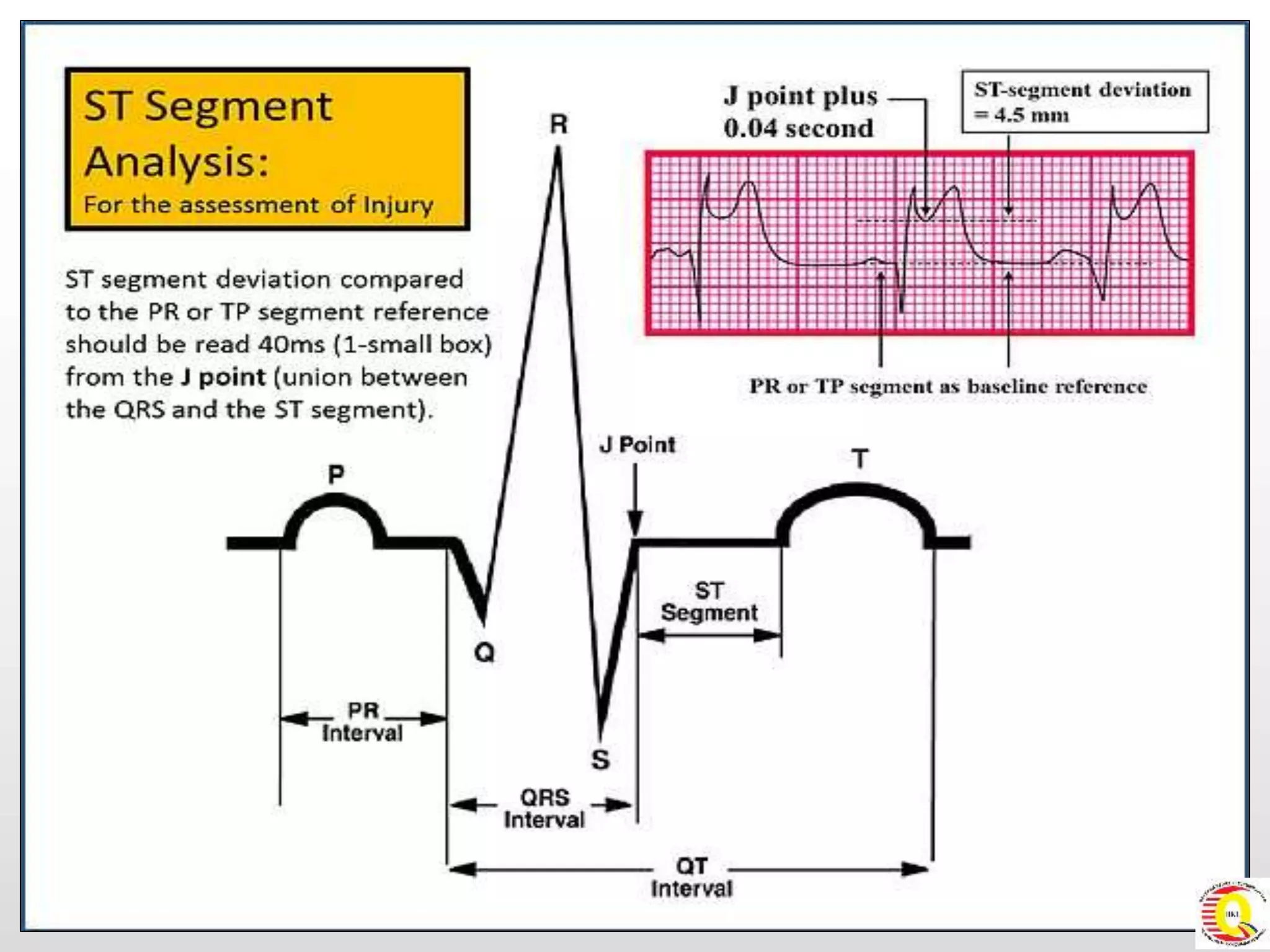
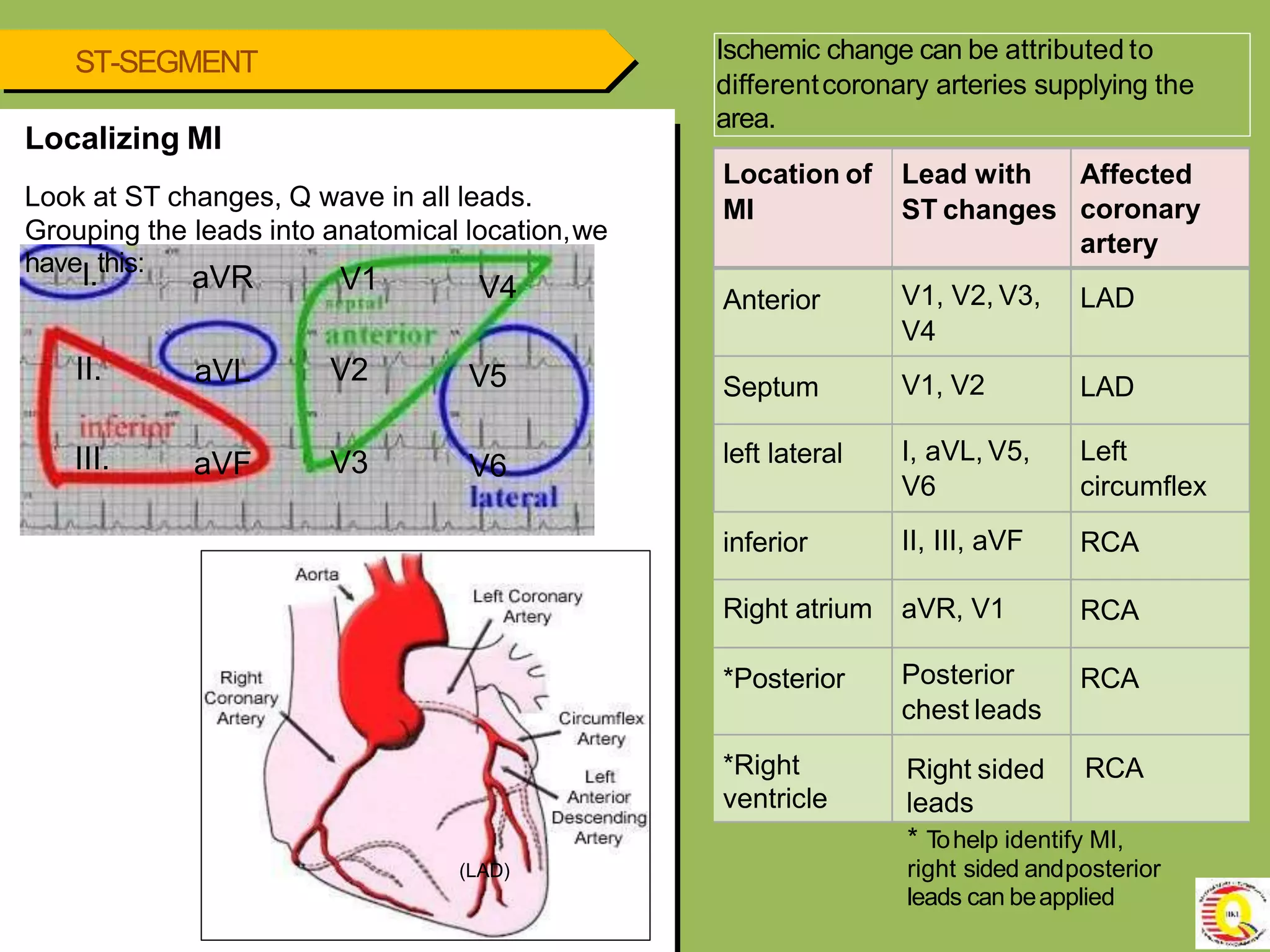
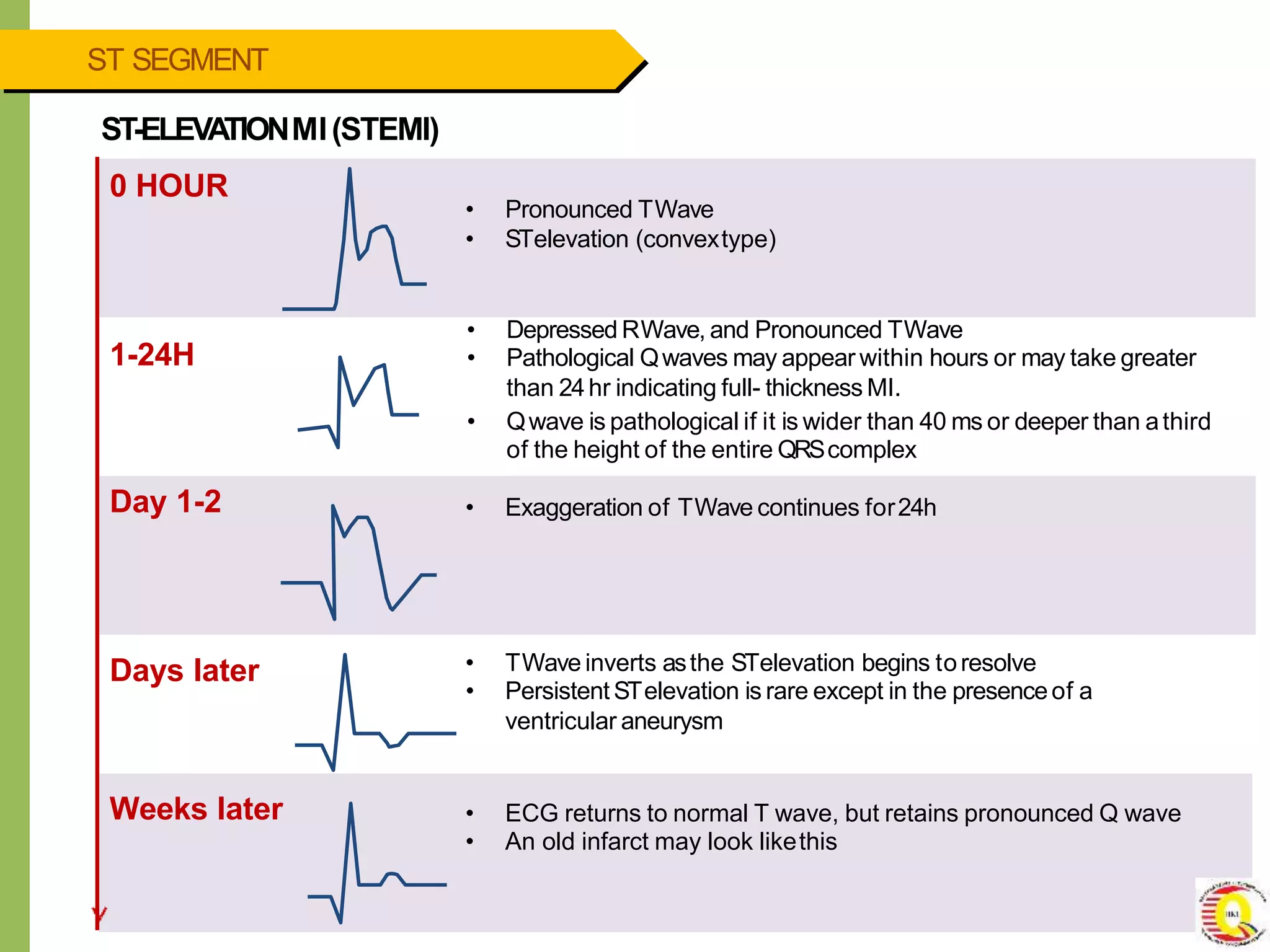
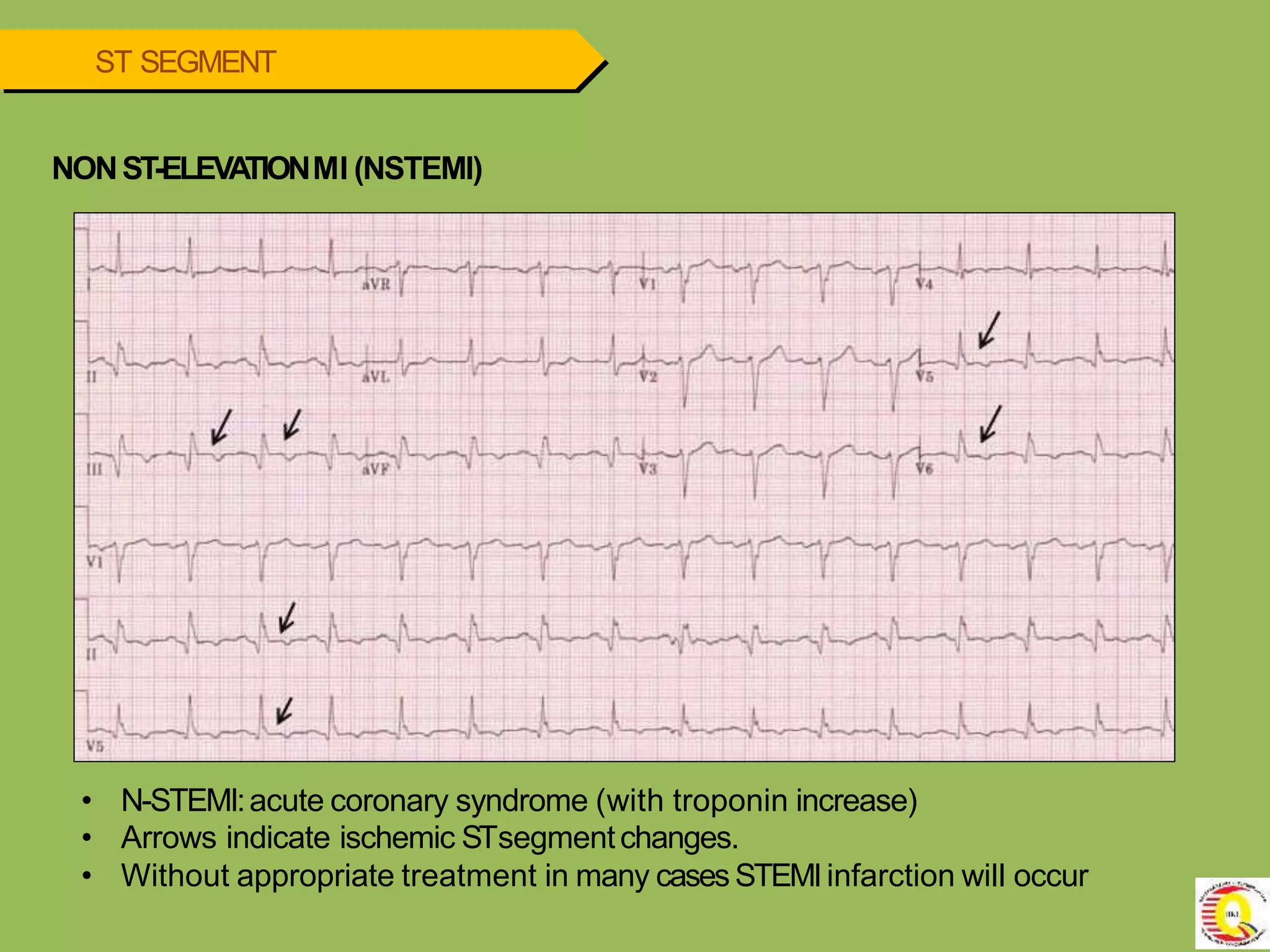
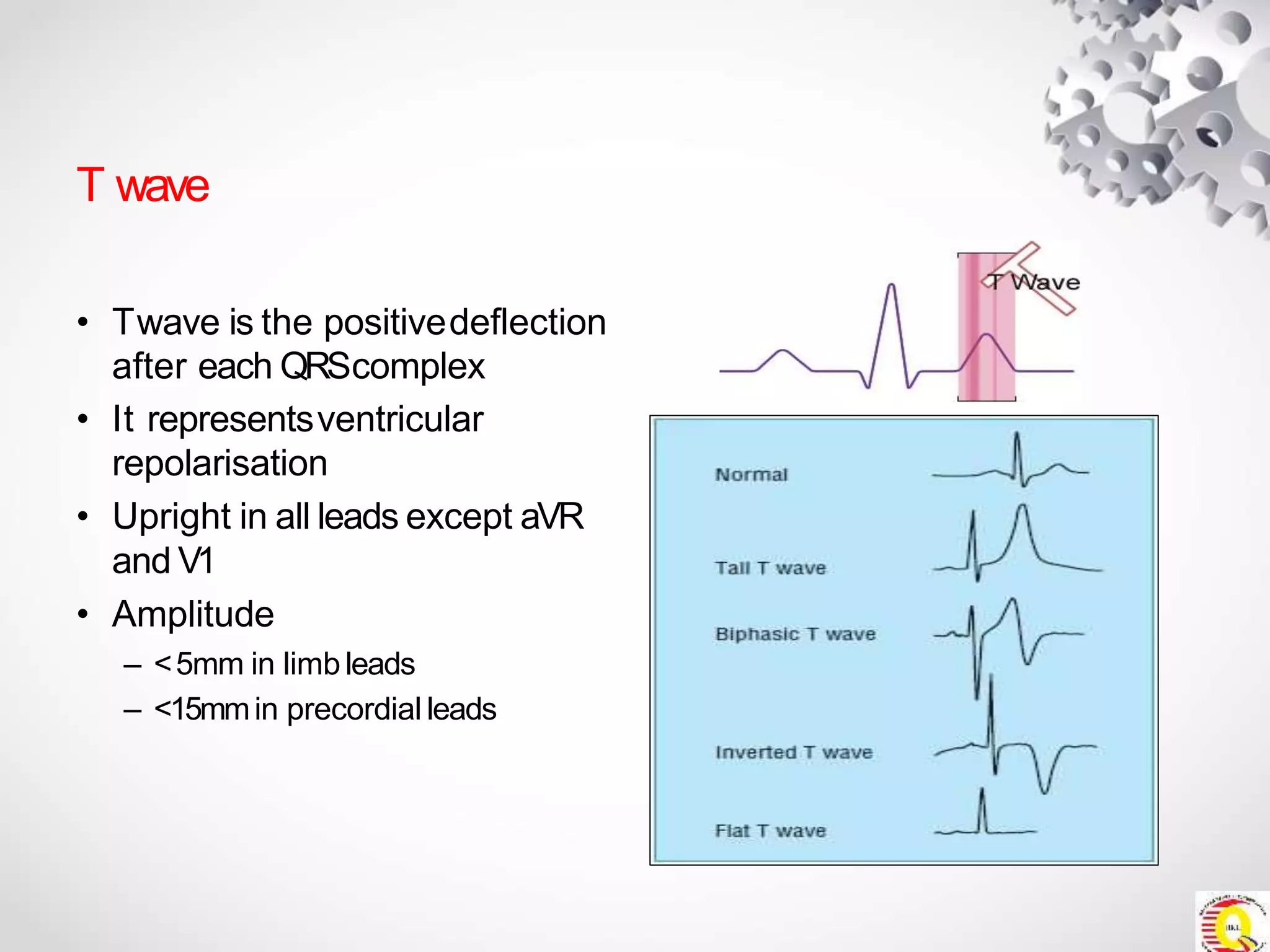
This document provides an overview of interpreting electrocardiograms (ECGs). It begins with the cardiac anatomy and conduction system. It then outlines a 6-step approach to ECG interpretation: 1) rate, 2) rhythm, 3) P-wave, 4) PR interval, 5) QRS complex, and 6) ST segment and T wave. Key aspects of normal and abnormal findings are defined for each step. Common conditions are discussed like sinus bradycardia, sinus tachycardia, atrial fibrillation, bundle branch blocks, myocardial infarction, and Wolff-Parkinson-White syndrome. The document emphasizes interpreting ECGs systematically and identifying both normal and abnormal tracings.