OVARIAN & UTERINECYCLE
•Starts at puberty - Menarche
•Normally continues until the Menopause.
•Reproductive cycles depend upon activities and coordination of :
Hypothalamus
Pituitary gland
Ovaries
Uterus
Uterine tubes
Vagina
Mammary Glands
3.
GnRH
Gonadotropins are thehormones produced to control the reproductive system.
The hormones involved are gonadotropin-releasing hormone (GnRH) secreted from the
hypothalamus, luteinizing hormone (LH) and follicle-stimulating hormone (FSH) produced by the
anterior pituitary gland and oestrogen and testosterone produced by the gonads. LH and FSH
are known as gonadotropins.
4.
REGULATION OF THEHPG AXIS
HYPOTHALAMUS – PITUITARY – GONADAL AXIS
The neurons in the hypothalamus form an interconnected network with other neural circuits of the brain,
allowing for integration of various signals, including light-dark cycles, body fat levels and stress.
GnRH acts on GnRH receptors found on gonadotroph cells of the anterior pituitary, stimulating the production
of two hormones:
•Luteinising Hormone (LH)
•Follicle Stimulating Hormone (FSH)
LH and FSH then act on the gonads (testes/ovaries), with differential effects.
5.
LUTEINIZING HORMONE INMALES
LH stimulates the Leydig cells in the testes to produce testosterone, the main male sex steroid hormone.
Testosterone has numerous effects, including:
•Stimulates formation of sperm (spermatogenesis) in the testes
•Maintenance of libido (sexual drive)
•Development of secondary sexual characteristics (pubic, axillary and facial hair)
•Growth of external genitalia
•Deepening of voice
•Muscle growth
•Bone growth
•Promotion of anabolic reactions
6.
FOLLICLE STIMULATING HORMONEIN
MALES
FSH drives sperm production in the Sertoli cells of the testes (spermatogenesis), as well as
synthesis of proteins important for the production and action of steroid hormones. They
include:
•Androgen binding protein (ABP) which maintains high levels of testosterone locally in the
luminal space of the seminiferous tubules.
•P450 aromatase, an enzyme that converts testosterone into oestradiol.
•Growth factors that support sperm cells and spermatogenesis, that result in increasing the
number of sperm cells, as well as promote motility and the fertility potential of sperm.
•Inhibins, which have a selective negative feedback effect on FSH only and not LH (i.e., inhibits
FSH production, but does not inhibit LH production). They also act as growth factors on Leydig
cells.
7.
FSH & LHHORMONES IN FEMALES
LH and FSH stimulate the ovary to produce mature gametes, as well as synthesise and secrete
oestrogens and progestins.
LH binds to theca cells on developing follicles as well as granulosa cells. After ovulation, LH binds to
cells of the. corpus luteum. It acts on theca cells to produce progestins and androgens. Androgens
enter granulosa cells and are then converted to oestrogens.
FSH binds to granulosa cells to:
•Increase production of enzymes that catalyse the production of steroid hormones, stimulating
follicle growth
•Increase production of activins, which have a positive feedback effect on the anterior pituitary
•Increase production of inhibins, which have a selective negative feedback effect on the pituitary
•Help convert androgens to oestrogen
9.
(+/-) Feedback inboth sexes.
A. In males, the Hypothalamic-Pituitary-Gonadal (HPG) axis is a negative feedback loop where testosterone and
inhibin B signal the hypothalamus and pituitary to reduce the release of gonadotropin-releasing hormone
(GnRH), luteinizing hormone (LH), and follicle-stimulating hormone (FSH)
B. In females oestrogens and progestins act on the anterior pituitary and the hypothalamus to
exert negative and positive feedback effects.
•Moderate oestrogen levels exert negative feedback on LH and FSH secretion
•High oestrogen levels (in the absence of progesterone) positively feedback on LH and FSH secretion
•Oestrogen in the presence of progesterone exerts negative feedback on the HPG axis
Progesterone is a sex steroid released by the corpus luteum, which is what the follicle turns into after the egg
has been released during ovulation.
FOLLICULAR PHASE
This isthe beginning of a new cycle as follicles (oocytes surrounded by stromal cells) begin to
mature and prepare to release an oocyte.
With very minimal hormone production the follicle begins to develop independently of
gonadotropins or ovarian steroids.
little negative feedback on HPG Axis
Only one dominant follicle can continue to maturity and complete each menstrual cycle. As
oestrogen levels rise, negative feedback reduces FSH levels, and only one follicle can survive,
with the other follicles becoming just polar bodies.
FSH
LH
STIMULATE
Follicle growth &
oestrogen production
LOW
Steriods
&
Inhibin
12.
OVULATION PHASE
LH SURGE
The follicle ruptures and
The mature oocyte is
assisted to the fallopian
tube by fimbria
It remains viable
for fertilization
for around 24
hours.
The follicle
remains luteinized,
secreting estrogen
and now
also progesterone
Reverts back a negative
feedback on the HPG axis
Together with
Inhibin inhibits
FSH
CYCLE PROCEEDS IN ANTICIPATION OF
FERTILIZATION
13.
LUTEAL PHASE
a. Tomaintain conditions for fertilization and implantation post ovulation,
B. In the absence of fertilization,
CORPUS LUTEUM
tissue in the ovary that forms
at the site of a ruptured
follicle
(produces ?)
Oestrogens
Progesterone
Inhibin
CORPUS LUTEUM regress
spontaneously after 14 days
significant fall
in hormones
Negative
Feedback is
relieved
HPG axis is
reset
PREPARES FOR THE NEXT CYCLE TO BEGIN
14.
CONTINUED..
c. If fertilizationoccurs,
At around 4 months of gestation, the placenta is capable of producing sufficient
steroid hormone to control the HPG axis.
The syncytiotrophoblast
of the embryo produces
human chorionic
gonadotropin (HCG)
Exerts a
luteinizing effect
& maintain
Corpus Luteum
Supported by placental
HCG and it produces
hormones to support
the pregnancy
16.
II. UTERINE CYCLE
Theuterine cycle, also known as the menstrual cycle, is a series of changes in
the lining of the uterus (endometrium) that occur in preparation for a potential
pregnancy.
It's a roughly 28-day cycle that involves menstruation, ovulation, and the
thickening of the uterine lining.
These changes are orchestrated by hormones like estrogen and progesterone.
17.
MENSES PHASE
Menses marksthe beginning of a new
menstrual cycle.
It occurs in the absence of fertilization once
the corpus luteum has broken down and the
internal lining of the uterus is shed.
Menstrual bleeding usually lasts between 2-7
days with 10-80ml blood loss.
18.
FOLLICULAR PHASE
The proliferativephase runs alongside the follicular
phase, preparing the reproductive tract for
fertilisation and implantation.
Oestrogen initiates fallopian tube formation,
thickening of the endometrium, increased growth
and motility of the myometrium and production of a
thin alkaline cervical mucus (to facilitate sperm
transport).
The follicular phase starts on the first day of the
period and lasts for 13 to 14 days.
Usually only one follicle will mature into an egg.
19.
OVULATION
It's the timewhen a woman is most fertile
This phase marks the release of a mature egg from
the ovary, usually around day 14 of a 28-day
cycle. .
20.
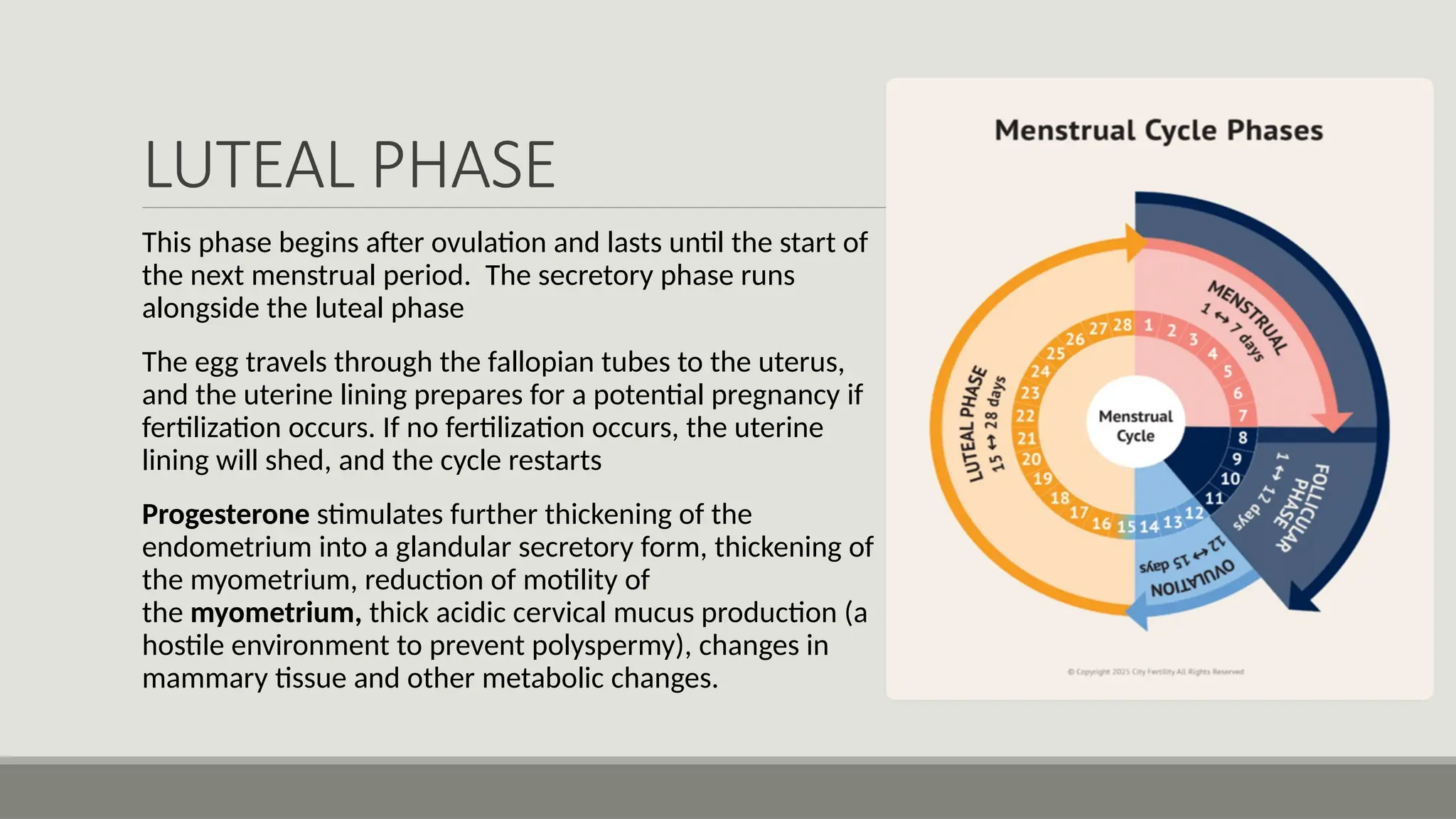
LUTEAL PHASE
This phasebegins after ovulation and lasts until the start of
the next menstrual period. The secretory phase runs
alongside the luteal phase
The egg travels through the fallopian tubes to the uterus,
and the uterine lining prepares for a potential pregnancy if
fertilization occurs. If no fertilization occurs, the uterine
lining will shed, and the cycle restarts
Progesterone stimulates further thickening of the
endometrium into a glandular secretory form, thickening of
the myometrium, reduction of motility of
the myometrium, thick acidic cervical mucus production (a
hostile environment to prevent polyspermy), changes in
mammary tissue and other metabolic changes.
21.
SUMMARY
The menstrual cycleis generally divided into four main phases:
a. menstruation,
b. the follicular phase,
c. ovulation, and
d. luteal phase
The cycle also involves the development of an egg and the thickening of the
uterine lining in preparation for potential pregnancy. If pregnancy doesn't occur,
the lining sheds during menstruation, and the cycle begins again.