Download to read offline
















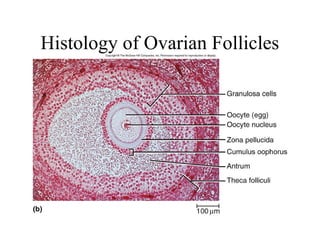













The document provides an overview of the male and female reproductive systems including: - Primary and secondary sex organs that produce and transport gametes in males (testes, ducts, glands) and females (ovaries, uterine tubes, uterus, vagina). - The hormonal regulation of the testes and ovaries, including feedback loops between the hypothalamus, pituitary gland, and gonads. - Spermatogenesis and oogenesis, the processes by which gametes are produced in the testes and ovaries. - The ovarian and uterine cycles regulated by hormones including estrogen and progesterone. Key events like ovulation and menstruation are described. - Fertilization and early embryonic development up





![Human reproduction By - Kalpana Wagh [MSc,BEd.]](https://cdn.slidesharecdn.com/ss_thumbnails/humanreproduction-200701060234-thumbnail.jpg?width=640&height=640&fit=bounds)













































![Atoms and molecules [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/atomsandmoleculesautosaved-160615024046-thumbnail.jpg?width=640&height=640&fit=bounds)























