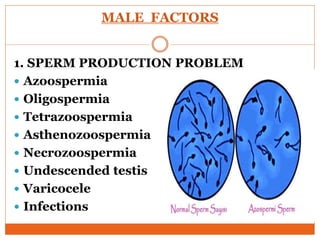
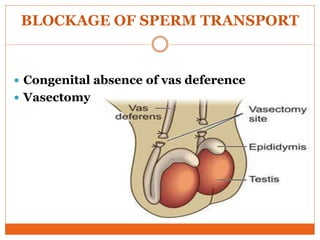
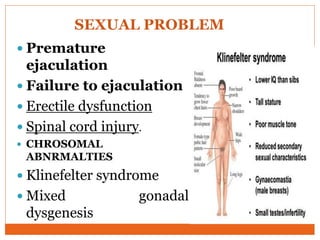
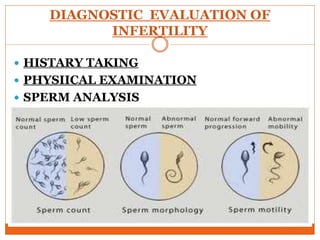
This document discusses infertility, including its definition, causes, diagnostic evaluation, and management. It notes that infertility is defined as the inability to conceive after one year of unprotected intercourse. The causes of infertility can be male factors related to sperm production or transport, female factors related to ovulation or egg/hormone problems, or combined factors in both partners. Diagnostic evaluation involves medical histories, physical exams, sperm analysis, hormone testing, imaging of reproductive organs, and other tests to identify treatable causes. Management depends on the underlying causes and may include lifestyle changes, surgery, assisted reproductive technologies like IVF, or alternatives to childbirth like adoption.