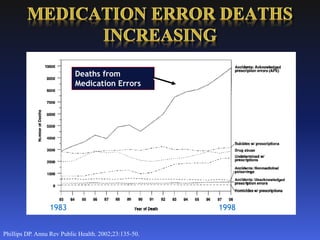
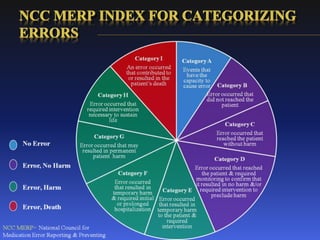
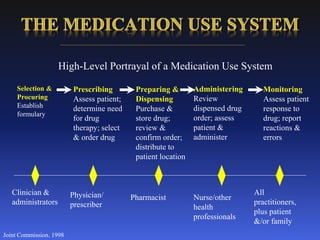
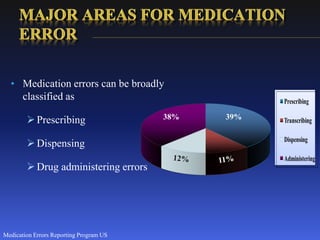
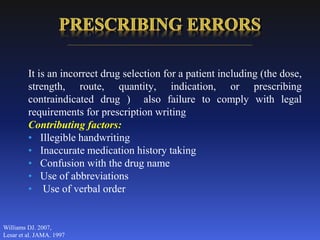
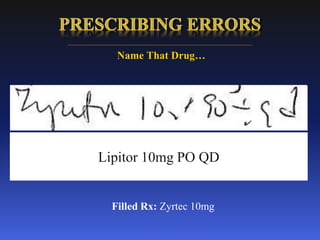


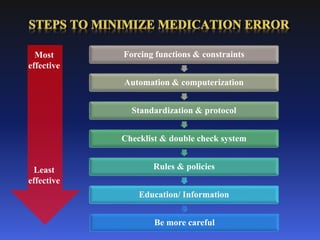

This document discusses medication errors, including definitions of key terms like adverse drug events and adverse drug reactions. It provides classifications and reasons for medication errors, as well as methods to prevent, identify, and minimize errors. These include implementing systems-based approaches, reducing reliance on memory through automation, standardizing processes, and employing checks and policies. Reporting of medication errors is also addressed.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












