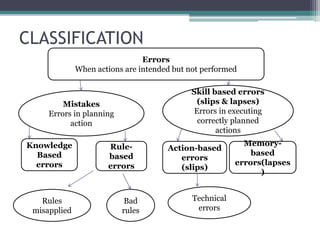
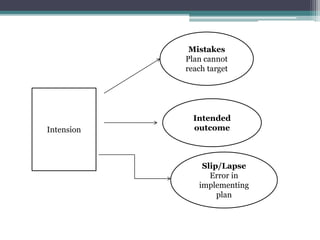
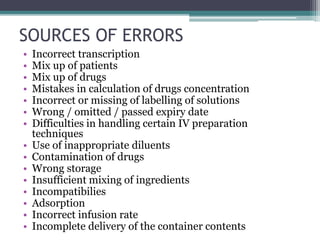
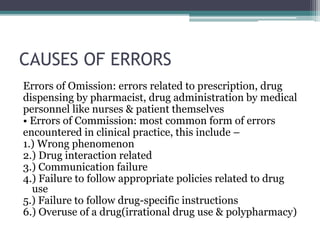
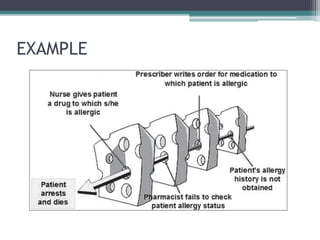
Medication errors are preventable events that may cause or lead to inappropriate medication use or patient harm. They can occur at any stage from prescribing to administration. Common factors that influence errors include lack of training, complex medication regimens, distractions, and look-alike drug names. Prescribing errors involve incorrect drug selection or dosing, while dispensing errors provide the wrong drug. Administration errors occur when the patient receives an incorrect medication. Reducing errors requires improved education, standardized processes, technology support like computerized prescribing, and checking procedures.