Download to read offline
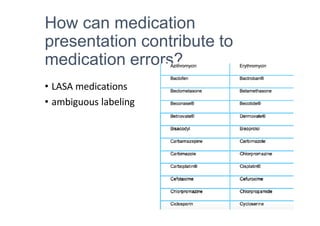

Medication safety is important to prevent patient harm from errors. Factors that contribute to errors include inadequate medication histories, lack of communication between providers, ambiguous labeling, and failure to double check medications. Efforts to improve safety include using generic names, tailoring prescriptions to each patient, knowing high-risk medications, developing checking habits, and encouraging patient involvement in their own care.