Downloaded 220 times

![Boxed Warning for All Prescription NSAIDs
Cardiovascular Risk
NSAIDs may cause an increased risk of serious cardiovascular thrombotic
events, myocardial infarction, and stroke, which can be fatal. This risk may
increase with duration of use. Patients with cardiovascular disease or risk
factors for cardiovascular disease may be at greater risk.
[Product] is contraindicated for the treatment of perioperative pain in the
setting of coronary artery bypass graft (CABG) surgery.
Gastrointestinal Risk
NSAIDs, including [product], cause an increased risk of serious
gastrointestinal adverse events including bleeding, ulceration, and
perforation of the stomach or intestines, which can be fatal. These events
can occur at any time during use and without warning symptoms. Elderly
patients are at greater risk for serious gastrointestinal (GI) events.
Cardiovascular Risk
NSAIDs may cause an increased risk of serious cardiovascular thrombotic
events, myocardial infarction, and stroke, which can be fatal. This risk may
increase with duration of use. Patients with cardiovascular disease or risk
factors for cardiovascular disease may be at greater risk.
[Product] is contraindicated for the treatment of perioperative pain in the
setting of coronary artery bypass graft (CABG) surgery.
Gastrointestinal Risk
NSAIDs, including [product], cause an increased risk of serious
gastrointestinal adverse events including bleeding, ulceration, and
perforation of the stomach or intestines, which can be fatal. These events
can occur at any time during use and without warning symptoms. Elderly
patients are at greater risk for serious gastrointestinal (GI) events.](https://image.slidesharecdn.com/tenprinciplesoa-151106074653-lva1-app6892/85/Ten-Principles-in-Osteoarthritis-Management-32-320.jpg)
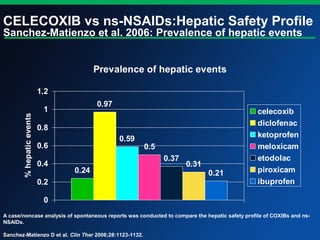

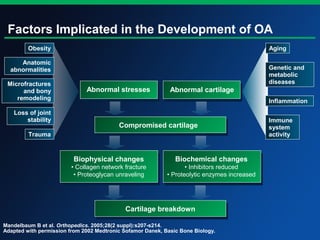
Osteoarthritis (OA) is a significant health concern affecting millions, with notable prevalence and burden in both the US and UK, leading to considerable disability. Effective management of OA must be patient-tailored and include both non-pharmacological (e.g., education, exercise) and pharmacological (e.g., NSAIDs, corticosteroids) strategies, while fostering an active doctor-patient relationship. Guidelines emphasize the importance of a comprehensive approach to reduce pain, improve quality of life, and limit disease progression.





































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



