






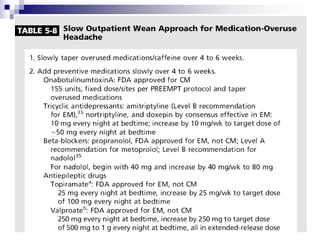


Medication-overuse headache (MOH) is a secondary chronic daily headache resulting from the overuse of analgesics and other acute headache medications, occurring 15 days/month for three months or more. It predominantly affects women and is commonly associated with migraine, leading to poorer quality of life. Treatment typically involves a detoxification process to improve responsiveness to future headache medications.




























































































