Hepatic
Encephalopathy.
Daniel Vela-Duarte, MD
Int. Medicine / Neurology
Loyola University Medical Center
2.
Case
62 yo male with h/o ESLD 2/2 NASH and 1AT def,
hepatorenal syndrome type II, DM II, who has presented
multiple admissions for altered mental status, alternating
somnolence, agitation and belligerence, diagnosed
subsequently with hepatic encephalopathy and treated
several times with large volume paracentesis and weekly
albumin infusions.
Pt was admitted for fluctuating changes in mental status,
anuria, noted worsening renal function, fluid overload,
hypotension and hemodialysis.
3.
Question …
What is the best treatment to
prevent recurrent hepatic
encephalopathy?
A. Lactulose 15ml BID / daily
B. Lactulose 15ml BID / daily + Rifaximin 550mg BID /daily
C. Rifaximin 550mg BID / daily
D. Lactulose 15ml BID during hospitalization
E. Neomycin 5 g / daily + Lactulose 15ml BID /daily
4.
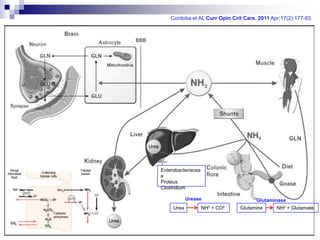
Cordoba et Al,Curr Opin Crit Care. 2011 Apr;17(2):177-83.
Enterobacteriacea
e
Proteus
Clostridium
Urease Glutaminase
Urea NH3 + CO2 Glutamine NH3 + Glutamate
5.
Back to theCase
Intravascularly depleteted
62 yo male with h/o ESLD 2/2 (Peripheral /splanchnic pooling)
NASH and 1AT def,
hepatorenal syndrome type II, DM II, who has presented
Renin-Angiotensin-Aldost.
multiple admissions for altered mental status, alternating
Na / water retention
somnolence, agitation and belligerence, diagnosed
subsequently with hepatic encephalopathy and treated
Intrarenal vasoconstriction
several times with large volumeATN ?
paracentesis and weekly
ESLD = Alb
albumin infusions. of Ammonia
-Impaired detox
Renal Perfusion
GFR
Pt was admitted for fluctuating changes in mental status,
anuria, noted worsening renal function, fluid overload,
hypotension and emergent hemodialysis.
Schepke M, Nephrol Dial Transplant (2007) 22 [Suppl 8]: viii2–viii4
6.
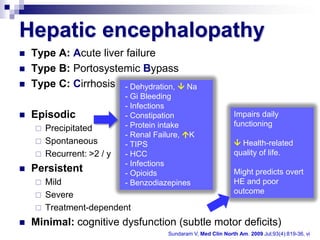
Hepatic encephalopathy
Type A: Acute liver failure
Type B: Portosystemic Bypass
Type C: Cirrhosis - Dehydration, Na
- Gi Bleeding
- Infections
Episodic - Constipation Impairs daily
- Protein intake functioning
Precipitated
- Renal Failure, K
Spontaneous - TIPS Health-related
Recurrent: >2 / y - HCC quality of life.
- Infections
Persistent - Opioids Might predicts overt
Mild - Benzodiazepines HE and poor
Severe outcome
Treatment-dependent
Minimal: cognitive dysfunction (subtle motor deficits)
Sundaram V, Med Clin North Am. 2009 Jul;93(4):819-36, vi
7.
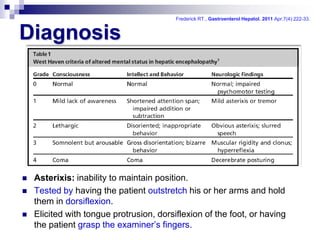
Frederick RT., GastroenterolHepatol. 2011 Apr;7(4):222-33.
Diagnosis
Asterixis: inability to maintain position.
Tested by having the patient outstretch his or her arms and hold
them in dorsiflexion.
Elicited with tongue protrusion, dorsiflexion of the foot, or having
the patient grasp the examiner’s fingers.
8.
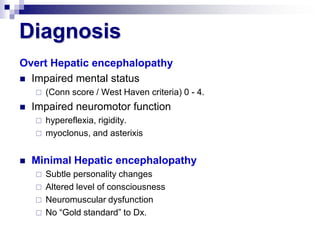
Diagnosis
Overt Hepatic encephalopathy
Impaired mental status
(Conn score / West Haven criteria) 0 - 4.
Impaired neuromotor function
hypereflexia, rigidity.
myoclonus, and asterixis
Minimal Hepatic encephalopathy
Subtle personality changes
Altered level of consciousness
Neuromuscular dysfunction
No “Gold standard” to Dx.
9.
Lactulose
It improves minimal HE, cognitive
functions and health-related quality of life
in cirrhotic patients.
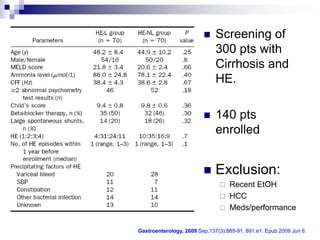
Is lactulose effective decreasing
recurrence of overt HE after recovery of
a previous episode?
10.
Screening of
300 pts with
Cirrhosis and
HE.
140 pts
enrolled
Exclusion:
Recent EtOH
HCC
Meds/performance
Gastroenterology, 2009 Sep;137(3):885-91, 891.e1. Epub 2009 Jun 6.
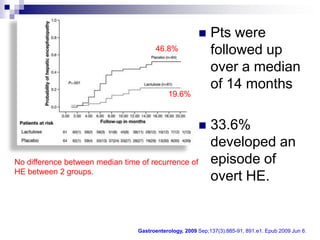
11.
Pts were
46.8% followed up
over a median
of 14 months
19.6%
33.6%
developed an
No difference between median time of recurrence of episode of
HE between 2 groups.
overt HE.
Gastroenterology, 2009 Sep;137(3):885-91, 891.e1. Epub 2009 Jun 6.
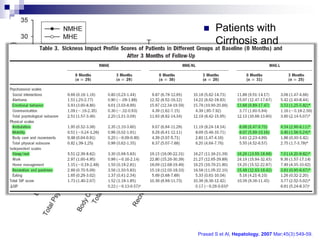
12.
Patients with
Cirrhosis and
MHE.
(No recurrent HE)
Improvement of
quality of life by
measurement of
SIP score
(Sickness impact
profile)
Prasad S et Al, Hepatology. 2007 Mar;45(3):549-59.
13.
Rifaximin
Efficacy and safety of rifaximin, for the
maintenance of remission from episodes
of HE in outpatients with a recent hx of
recurrent, overt HE (Prevention for 6m)
14.
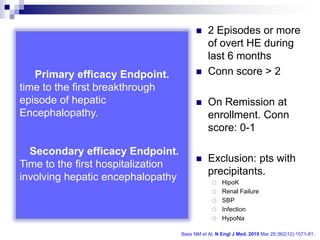
2 Episodes or more
of overt HE during
last 6 months
Primary efficacy Endpoint. Conn score > 2
time to the first breakthrough
episode of hepatic On Remission at
Encephalopathy. enrollment. Conn
score: 0-1
Secondary efficacy Endpoint.
Exclusion: pts with
Time to the first hospitalization
precipitants.
involving hepatic encephalopathy HipoK
Renal Failure
SBP
Infection
HypoNa
Bass NM et Al, N Engl J Med. 2010 Mar 25;362(12):1071-81.
15.
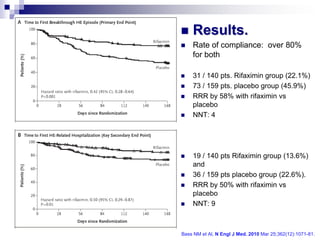
Results.
Rate of compliance: over 80%
for both
31 / 140 pts. Rifaximin group (22.1%)
73 / 159 pts. placebo group (45.9%)
RRR by 58% with rifaximin vs
placebo
NNT: 4
19 / 140 pts Rifaximin group (13.6%)
and
36 / 159 pts placebo group (22.6%).
RRR by 50% with rifaximin vs
placebo
NNT: 9
Bass NM et Al, N Engl J Med. 2010 Mar 25;362(12):1071-81.
16.
Conclusions
Rifaximin reduces the risk of a breakthrough episode of
HE by 58% vs placebo (Lactulose only) during the at
least 6 months of treatment.
Rifaximin reduces the risk of a hospitalization involving
HE by 50% vs placebo (Lactulose only) during the at
least 6 months of treatment.
Lactulose: 30 -60 ml / 2-3 doses, improves cognitive
functions in patients with minimal HE after 3 months of
treatment.
Lactulose: 30 -60 ml / 2-3 doses, decreases the
incidence of recurrent HE (RRR 58%)
![Back to the Case
Intravascularly depleteted
62 yo male with h/o ESLD 2/2 (Peripheral /splanchnic pooling)
NASH and 1AT def,
hepatorenal syndrome type II, DM II, who has presented
Renin-Angiotensin-Aldost.
multiple admissions for altered mental status, alternating
Na / water retention
somnolence, agitation and belligerence, diagnosed
subsequently with hepatic encephalopathy and treated
Intrarenal vasoconstriction
several times with large volumeATN ?
paracentesis and weekly
ESLD = Alb
albumin infusions. of Ammonia
-Impaired detox
Renal Perfusion
GFR
Pt was admitted for fluctuating changes in mental status,
anuria, noted worsening renal function, fluid overload,
hypotension and emergent hemodialysis.
Schepke M, Nephrol Dial Transplant (2007) 22 [Suppl 8]: viii2–viii4](https://image.slidesharecdn.com/cqc-hepaticencephalopathy-120616004807-phpapp01/85/Hepatic-encephalopathy-5-320.jpg)