Download as PDF, PPTX




![ Oral progestin dydrogesterone , compared with
placebo or supportive care (eg, bed rest)
significant decrease in the rate of miscarriage in
the progestin group (13 vs 24%; odds
ratio [OR] 0.47, 95% CI 0.310.7).
[Carp, 2012 MA].
Limitation:
small number of participants and events
poor methodologic quality of studies
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-12-320.jpg)
![Bed rest
commonly recommended
unnecessary and will not affect outcome
RCT: bed rest at home or in the hospital is not
beneficial in preventing fetal loss
[Aleman et al, 2005].
Abstinence from sexual intercourse and physical
exertion
typically advised
no data to support this.
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-15-320.jpg)
![Choosing a treatment method
Surgical (dilation and curettage) or
Medication (misoprostol)
Expectant management.
All have similar efficacy
Choice depends mainly upon patient preference.
[Sotiriadis et al, 2005MA].
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-17-320.jpg)






![Dose:
Single is preferred
1. Single and repeated doses of oral misoprostol
600 ug (with the dose repeated after 4 hours to a
total of 1 200 ug):
equally effective
diarrhoea is less.
(Nguyen et al, 2005)
2. The expulsion rate: higher with a single dose of 600
to 800 mcg given vaginally (70 to 90%)
{local effect of misoprostol on the uterine cervix, the high
drug concentration achieved in uterine tissue, and the
increased bioavailability with vaginal administration].
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-34-320.jpg)
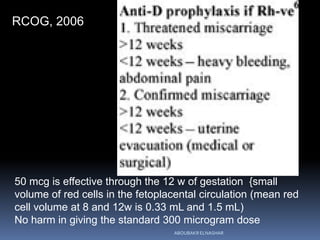
![Incomplete abortion
Oral: 600 ug (single dose)
[WHO, 2007]
Vaginal: 800ug
Oral : 400 μg.
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-36-320.jpg)
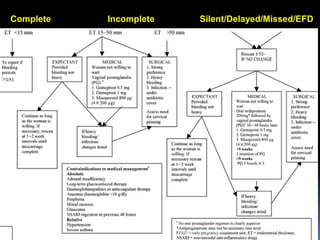
![Silent, delayed, missed miscarriage or
early fetal demise
•Vaginal: 800 ug per or
•Sublingual: 600 ug(single dose)
[WHO, 2007]
oral, sublingual or vaginal
400, 600 or 800 g in single or repeated doses
Sublingual: 400 g appears to be a safe, effective
alternative to the oral or vaginal routes.
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-37-320.jpg)
![Surgical advantages:
1. Shorter time to completion of tt.
complete evacuation within 48 h is more likely with surgical
than medical and more likely with medical than expectant
[Sotiriadis et al, 2005MA].
2. lowers risk of unplanned hospital admissions and
need for subsequent tt.
(MIST (Miscarriage treatment trial) randomized trial, the only trial to
compare all three treatment strategies: E, M, S
[Trinder et al, 2006])
(49 vs 18 vs 8%).
Further Surgical intervention
(44 vs13 vs 5%)
3. Blood transfusions
(2 vs, 1vs 0%)
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-42-320.jpg)

![3. Ultrasound
Criteria for an empty uterus:
homogeneous intrauterine dimension ≤11 cm in
combined transverse and sagittal planes
[Leung et al, 2006].
Indication of evacuation:
retained tissue with a diameter ≥15 mm .
Using the latter criteria, 5% of women had complications, and 40% required another
intervention (medical or surgical). However, there is also evidence that increased endometrial
thickness is not predictive of morbidity in asymptomatic women (Creinin et al, 2004)
If the ultrasound reveals retained tissue and the patient is asymptomatic or having only
minimal bleeding, we offer the patient surgical evacuation of the uterus or expectant
management for another two weeks.
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-57-320.jpg)


![V. Interval to conception
To postpone for 2-3 months: not advised
{no greater risk of adverse outcome with a shorter
interpregnancy interval
(Goldstein et al, 2004).
In one prospective study (n = 677), the overall rates
of live birth, miscarriage, and other pregnancy
complications after a pregnancy loss among women
with interpregnancy interval of ≤3 months and >3
months were similar}
[Makhlouf et al, 2014].
ABOUBAKR ELNASHAR](https://image.slidesharecdn.com/miscaraigemanagement-151002202420-lva1-app6891/85/Management-of-first-trimester-miscarriage-66-320.jpg)


This document discusses the management of first trimester miscarriage. It defines miscarriage as pregnancy loss before 20 weeks of gestation. For threatened miscarriage of a viable pregnancy, bed rest is not recommended as it does not affect outcomes. Oral progestins may help reduce miscarriage risk but evidence is limited. For non-viable pregnancies, expectant management, medical treatment with misoprostol, or surgical dilation and curettage are options based on patient preference and circumstances. Medical treatment involves administering misoprostol vaginally or orally in single or repeated doses depending on the type of miscarriage.

































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









