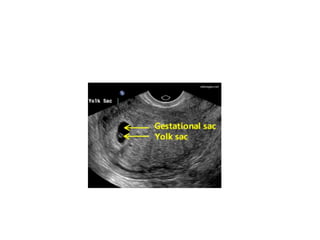
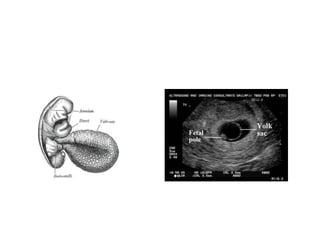
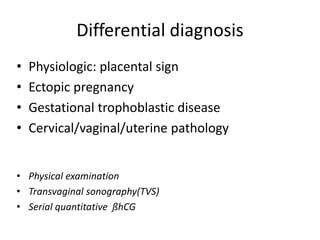
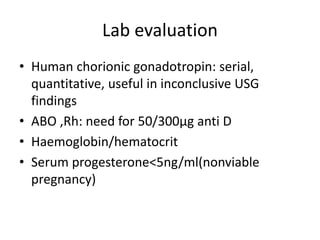
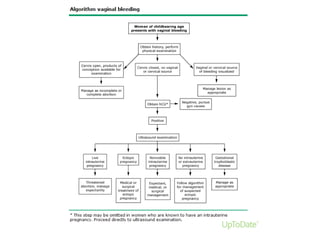
Spontaneous abortion, also known as miscarriage, is the unplanned expulsion or extraction of an embryo or fetus before 20 weeks of gestation. Risk factors include advanced maternal age, previous spontaneous abortions, smoking, and certain medications. Most spontaneous abortions are due to fetal chromosomal or structural abnormalities. Clinically, women present with vaginal bleeding and pelvic pain. Diagnosis involves pelvic examination, ultrasound criteria for gestational sac size and fetal heart activity. Treatment options include expectant management, medical methods using misoprostol, or surgical evacuation. Prevention focuses on preconception counseling and screening, and treating underlying maternal conditions.



















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

