- Stillbirth is defined as fetal death occurring after 20 weeks of gestation or a fetal weight of at least 500 grams. The worldwide stillbirth rate is over 3 million per year.
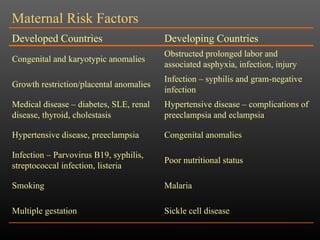
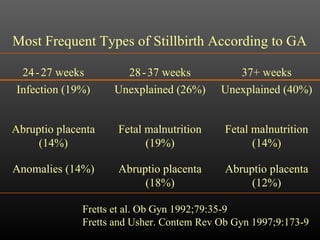
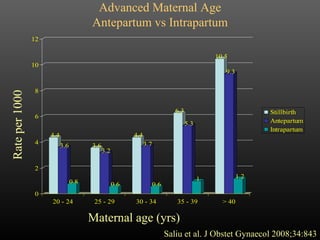
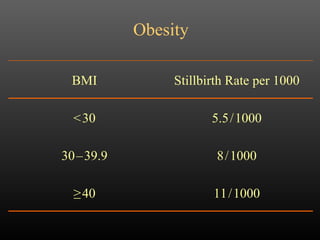
- The causes of stillbirth are often unknown, but may include maternal conditions like diabetes or hypertension, fetal conditions like growth restriction, and placental conditions like abruption. Advanced maternal age, obesity, and multiple gestations are also risk factors.
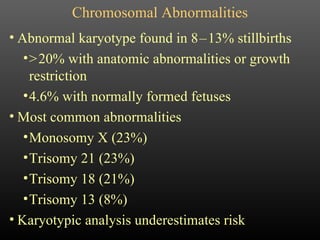
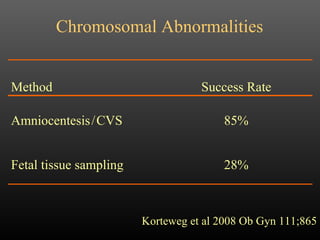
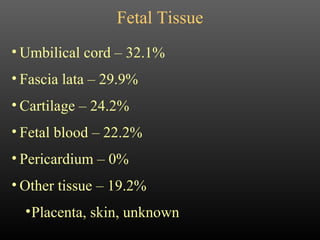
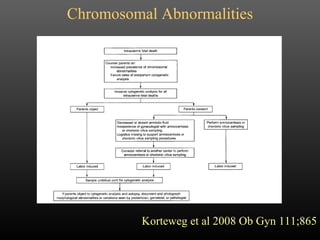
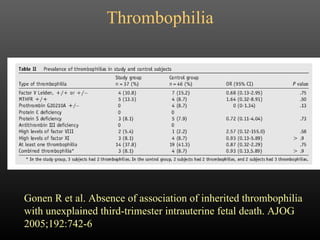
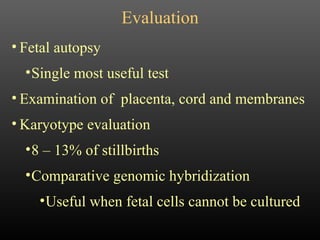
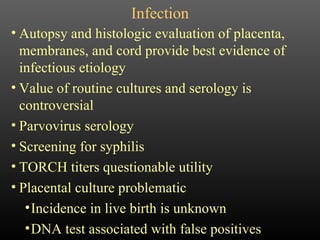
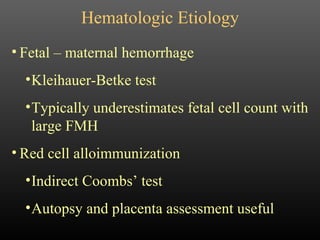
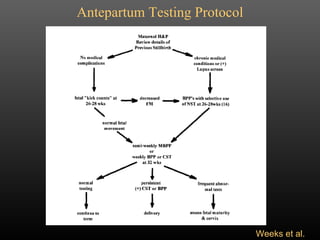
- Evaluation of stillbirth includes fetal autopsy, placental examination, and genetic testing. However, the optimal testing and management for subsequent pregnancies after an unexplained stillbirth remains uncertain due to lack of evidence.























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











