Download as PDF, PPTX
















![A. Before pregnancy: Pre-conceptional
counseling
1. Clinical: review med and obs history, asses other
risk factors, obesity, age
2. Lab:
Confirm persistent aPLab
Assess R function
CBC: anaemia thrompocytopenia
3. Treatment
Postpone pregnancy if thrombotic event <6 month
Initial low dose aspirin [increase success]Aboubakr Elnashar](https://image.slidesharecdn.com/antiphospholipidsynd-140806050613-phpapp01/75/Obstetric-antiphospholipid-antibody-syndrome-21-2048.jpg)













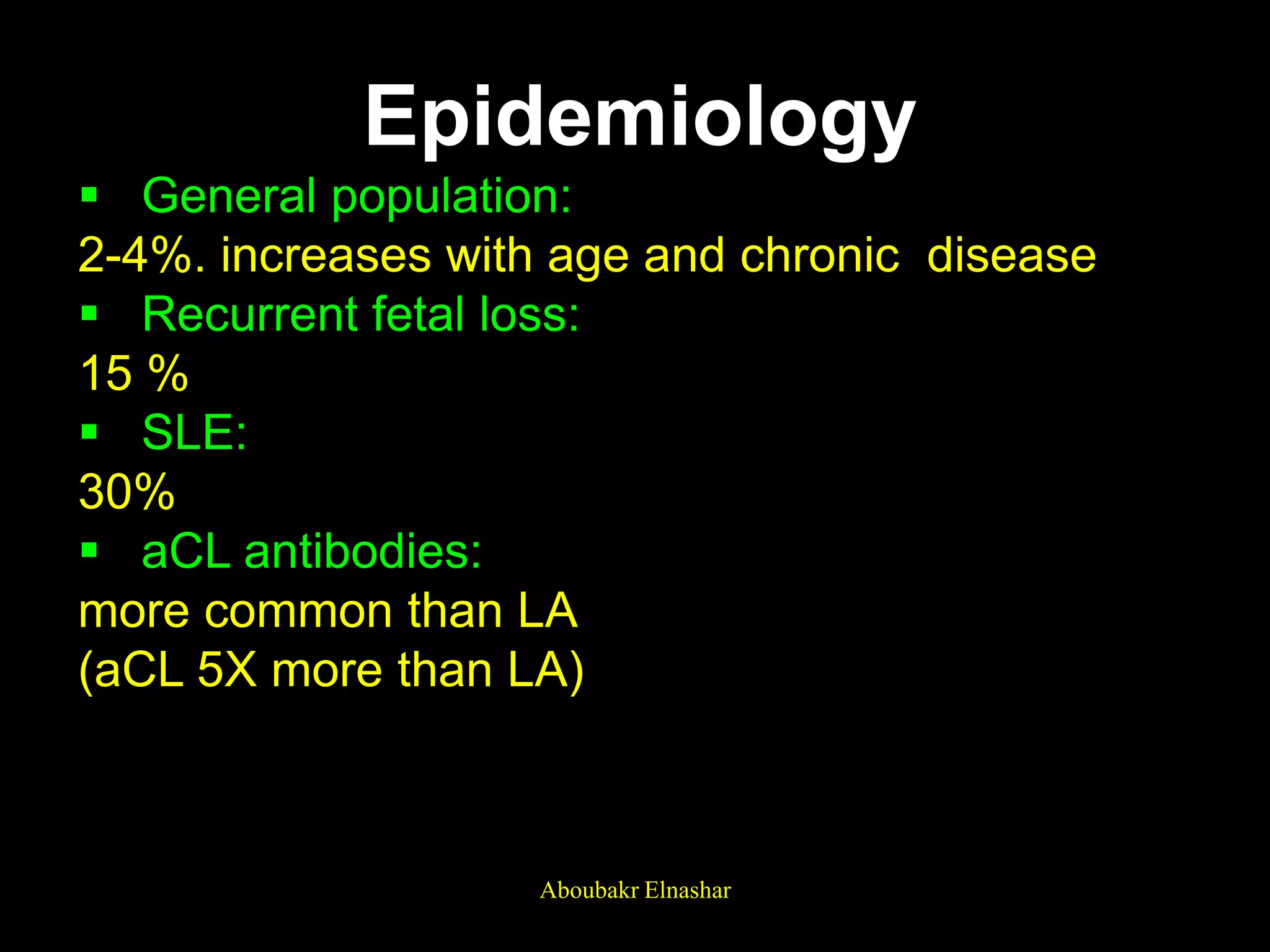
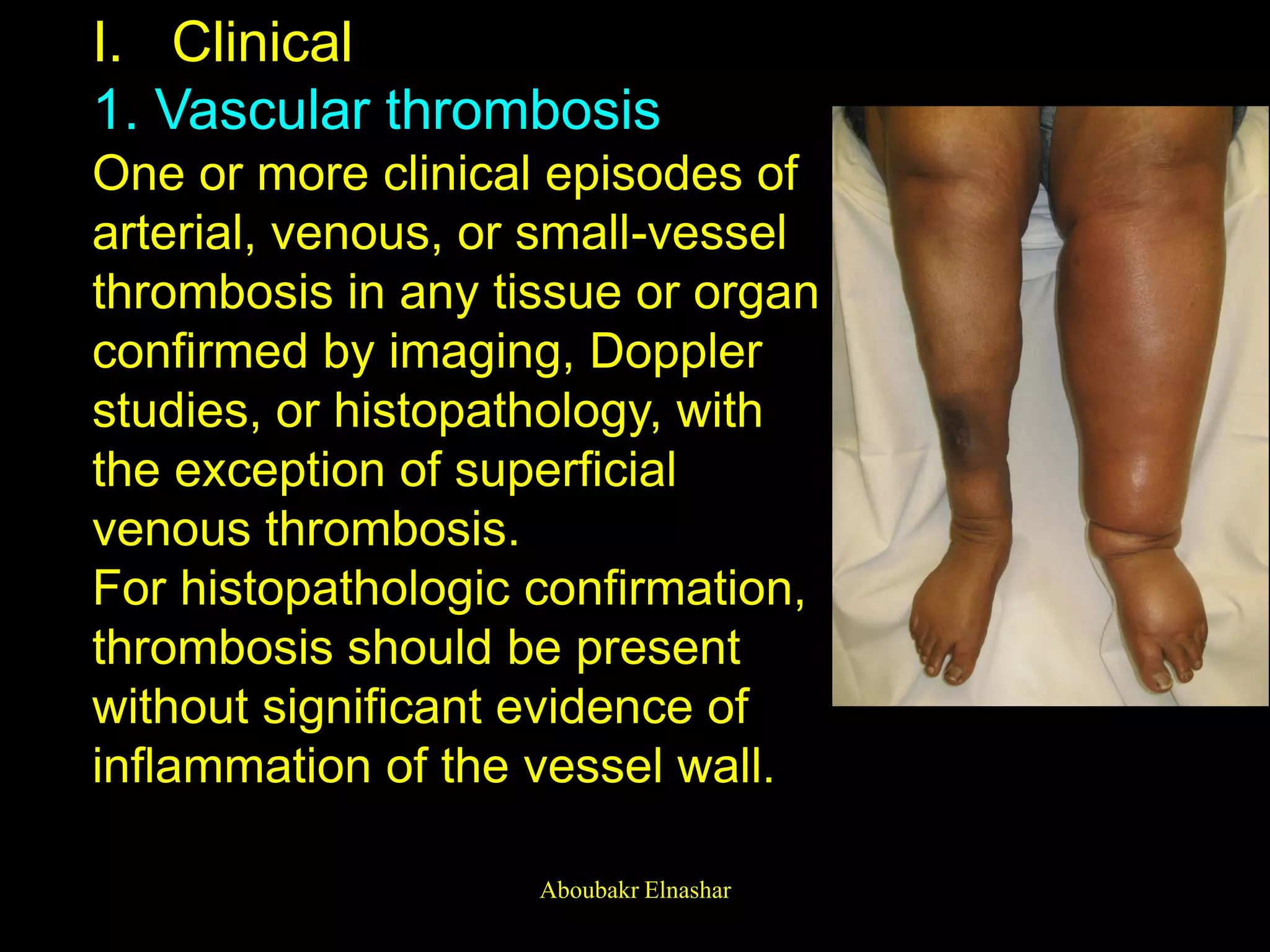
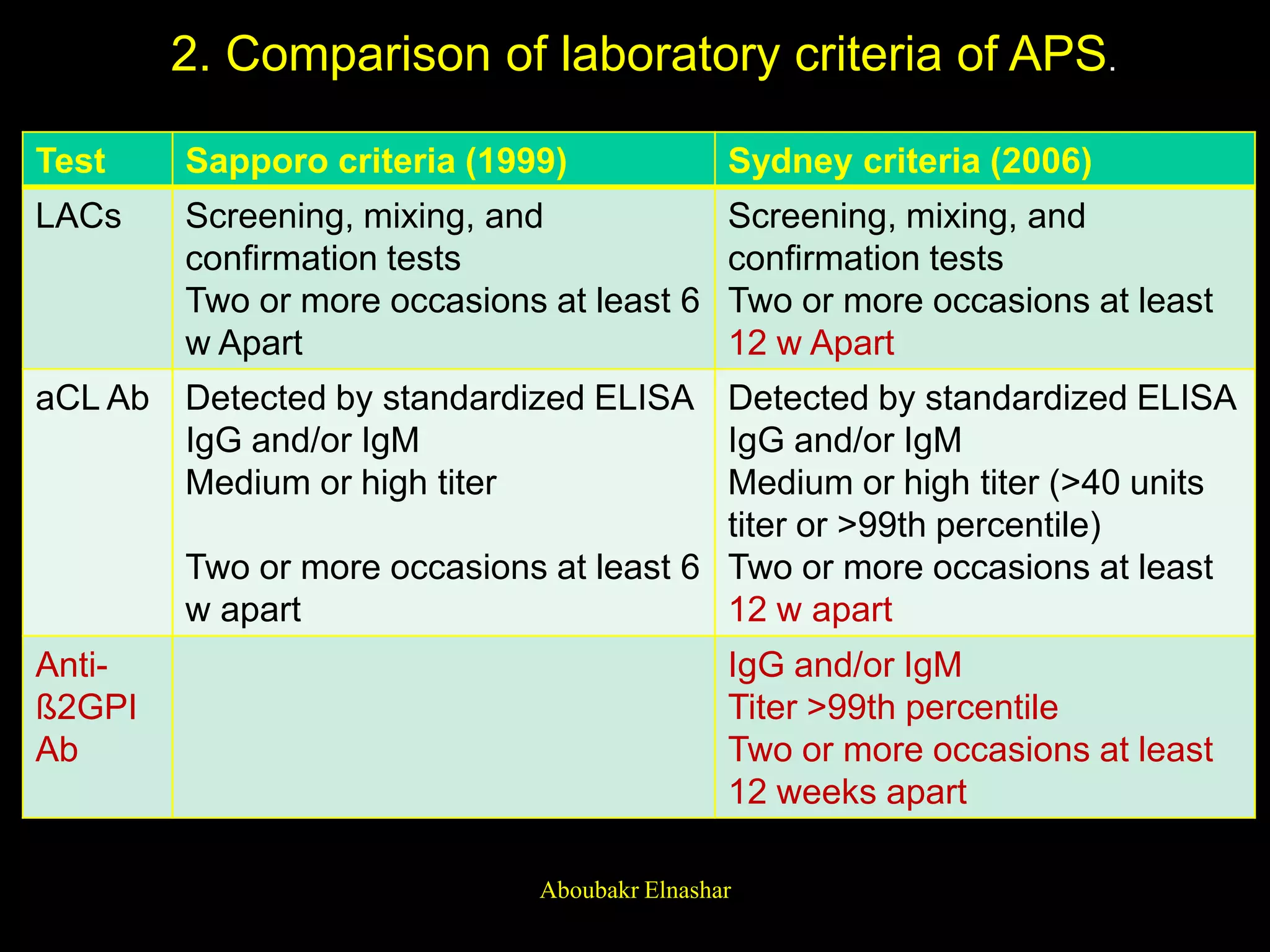
1. Antiphospholipid syndrome (APS) is an autoimmune disorder characterized by arterial or venous thrombosis or pregnancy morbidity in the presence of antiphospholipid antibodies. 2. The diagnosis requires one clinical criterion of vascular thrombosis or pregnancy complications and one laboratory criterion of positive testing for antiphospholipid antibodies on two occasions at least 12 weeks apart. 3. Treatment during pregnancy involves low-dose aspirin and heparin starting at a positive pregnancy test through 34 weeks gestation to reduce the risk of pregnancy complications like miscarriage, preeclampsia, and intrauterine growth restriction.