Definition
• Clinically recognisedpregnancy loss before
20th
week of gestation
• Expulsion or extraction of an embryo or fetus
weighing 500gm or less(WHO)
3.
Incidence
• MC earlypregnancy complication
• Frequency decreases with increasing
gestational age
• Incidence:8-20%(clinically recognised
pregnancies)
• Women who had a child: 5% incidence of
miscarriage
• 80% spontaneous abortion :< 12 wks
4.
Risk factors
• Advancedmaternal age
• Previous spontaneous abortion
• Medications & substances (smoking)
• Mechanisms responsible for abortion: not
apparent
• Death of fetus precedes spont. expulsion,
finding cause involves ascertaining the cause
of fetal death
5.
Maternal age
• Mostimportant risk factor in healthy women
• 30yrs:9-17%
• 35yrs:20%
• 40yrs:40%
• 45yrs: 80%
Medications or substances
•Heavy smoking(>10 cigarettes/day) :
vasoconstrictive & antimetabolic effects of
tobacco smoke
• Moderate to high alcohol consumption(>3
drinks/week)
• NSAIDS use(acetaminophen) :abnormal
implantation & pregnancy failure due to
antiprostaglandin effect
8.
Other factors
• Lowplasma folate levels(≤2.19ng/ml): no
specific evidence to support
• Extremes of maternal weight: prepregnancy
BMI<18.5 OR >25kg/m2
• Maternal fever:100°F(37.8°C), no evidence to
support
Clinical presentation
• Vaginalbleeding
– Scant brown spotting to heavy vaginal bleeding
– Amount /pattern does not predict outcome
– May be accompanied by passage of fetal tissue
• Pelvic pain
– Crampy /dull in character
– Constant/intermittent
• Incidental finding on pelvic ultrasound in
asymptomatic patient
13.
Diagnostic evaluation
• History
–Period of amenorrhea ,LMP/USG
• Physical examination: Complete pelvic
examination:
– P/S,:source, amount of bleeding, dilated cervix,
POC visible at Os/in vagina
– P/V: uterine size(consistent with GA)
• Pelvic ultrasound
14.
Pelvic ultrasound
• Mostuseful test in diagnostic evaluation of
women with suspected spontaneous abortion
• Foetal cardiac activity: most important (5.5-
6wks)
• Foetal heart rate
• Size & contour of G.sac
• Presence of yolk sac
• Best evaluated ,transvaginal approach(TVS)
15.
Pelvic USG: criteriafor spontaneous
abortion
• Gestational sac ≥ 25mm in mean diameter
that does not contain a yolk sac or embryo
• An embryo with CRL ≥7 mm with no cardiac
activity
If the GS or embryo is smaller than these dimensions:
repeat pelvic USG in 1-2 weeks
Lab evaluation
• Humanchorionic gonadotropin: serial,
quantitative, useful in inconclusive USG
findings
• ABO ,Rh: need for 50/300µg anti D
• Haemoglobin/hematocrit
• Serum progesterone<5ng/ml(nonviable
pregnancy)
18.
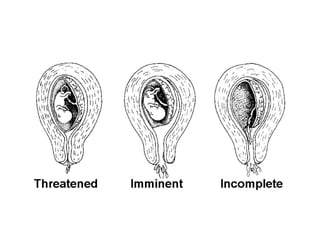
Post diagnostic classification
•Based upon the location of POC
• Degree of cervical dilatation(pelvic exam)
• Pelvic ultrasound
• Categorization impacts clinical management
– Threatened
– Inevitable
– Incomplete/complete
– Missed
19.
Threatened abortion
• Vaginalbleeding has occurred
• The cervical os is closed
• Diagnostic criteria for spontaneous abortion
has not met
• Managed expectantly: until symptoms resolve
or progresses
20.
Threatened abortion: m/m
•Expectant
• Progestin treatment: most promising, efficacy
not established
• Bed rest: randomised trials have refuted the
role
• Avoid vigorous activity
• Avoid heavy lifting
• Avoid sexual intercourse
21.
Threatened abortion :m/m
•Counsel about risk of miscarriage
• Return to hospital in case of additional vaginal
bleeding, pelvic cramping or passage of tissue from
vagina
• Repeat pelvic USG until a viable pregnancy is
confirmed or excluded
• Viable pregnancy, resolved symptoms: prenatal care
• If symptoms continue: monitor for progression to
inevitable, incomplete, or complete abortion
22.
Inevitable abortion
• Vaginalbleeding, typically accompanied by
crampy pelvic pain
• Dilated cervix( internal os)
• Products of conception felt or visualised
through the internal os
23.
Incomplete abortion
• Vaginalbleeding and/or pain present
• Cervix is dilated
• Products of conception partially expelled out
• Uterine size less than period of amenorrhea
24.
Missed abortion
• Nonviable intrauterine pregnancy
• Cervical os is closed
• POC not expelled
• May notice that symptoms associated with
early pregnancy have abated
26.
Management
• Complete evacuationof uterine
contents(POC)
• Surgical methods: suction evacuation/suction
curettage/dilation & evacuation
• Medical methods: Misoprostol,mifepristone
• Expectant
• All have similar efficacy
Medical methods
• Misoprostol:drug of choice
• Efficacy depends on dose & route of
administration
• 400mcg vaginally every 4 hours for 4 doses
• Expulsion rate : 50-70%
• Low cost, low incidence of side effects, stable
at room temperature, readily available, timing
of use can be controlled by patient
29.
Misoprostol
• WHO consensusreport on misoprostol
regimen
– Missed abortion: 800mcg vaginally,or 600 mcg
sublingually
– Incomplete abortion: 600mcg orally
• Expulsion rate: 70-90%
30.
Choosing the method
•Surgical evacuation : heavy bleeding,
intrauterine sepsis, medical co morbidities,
misoprostol is contraindicated
– Shorter time to completion of treatment
– Lowers risk of unplanned admissions
– Lower need for subsequent treatment
32.
Expectant m/m
• Stablevital signs
• No evidence of infection
• Offered after proper counseling
• If unsuccessful after 4 wks ,surgical evacuation
is needed
33.
Complete abortion
• POCexpelled completely from uterus &
cervix
• Cervical os is closed
• Uterus small in size (GA)
• Resolved or minimal vaginal bleeding & pain
• Aim of t/t: ensure that bleeding is not
excessive & all POC have expelled
• Theoretically does not need treatment




































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



