Bleeding in earlypregnancy
Dr. Alaa Nadhim Hameed
Republic of Iraq Ministry of higher education and scientific research
Kirkuk university
College of medicine
Republic of Iraq Ministry of higher education and scientific research
Kirkuk university
College of medicine
3.
Learning objectives
To knowthe definition of miscarriage
To know causes of Miscarriage
To understand clinical presentation & investigation
To know the types of Miscarriage
To understand the management options
Miscarriage
Spontaneous loss ofa pregnancy prior to viability, 23 weeks and
6 days of gestation.
• Beyond this gestation,fetal demise is classified as a stillbirth.
• The majority of first‐trimester miscarriages occur below 12
weeks’ gestation with an overall rate of around 20%.
• Second‐trimester miscarriages are less common, accounting
for 1–4% of all miscarriages
E
6.
First‐trimester miscarriage
• Itis thought that up to 95% of chromosomally abnormal embryos
result in miscarriage
• Trisomies: 68%, mainly trisomy 16, 21 and 22.
• Triploidy: 17.1%.
• Monosomy: 9.8% (XO Turner’s syndrome).
Other causes implicated in first‐trimester miscarriage include the
following.
• Maternal disease: antiphospholipid syndrome, diabetes,thyroid disease.
• Drugs: methotrexate, some antiepileptic drugs.
• Uterine abnormalities: the role of fibroids is uncertain but they may be implicated [5].
• Infection: varicella, rubella and other viral illnesses
&
7.
Second‐trimester miscarriage
• Cervix:cervical injury from surgery, cone biopsy and large loop excision of
the transformation zone.
• Infection: may occur with or without ruptured membranes.May be local to
the genital tract or systemic.
• Thrombophilias.
• Uterine abnormalities: submucous fibroids and congenital distortion of the
cavity (uterine septa) may be implicated.
• Chromosomal abnormalities: these too may not become apparent until
the second trimester.
&
8.
History
Typical symptoms ofmiscarriage include:
-Vaginal bleeding
-Cramping abdominal pain
-Passage of fetal tissue or clots
Other important areas to cover in the history include:
- LMP
- Cause if present
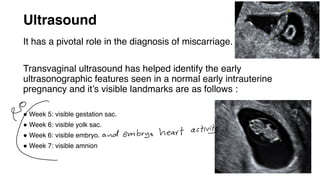
Ultrasound
It has apivotal role in the diagnosis of miscarriage.
Transvaginal ultrasound has helped identify the early
ultrasonographic features seen in a normal early intrauterine
pregnancy and it’s visible landmarks are as follows :
● Week 5: visible gestation sac.
● Week 6: visible yolk sac.
● Week 6: visible embryo.
● Week 7: visible amnion
9) and embryo heart activit
Other categories ofmiscarriage and abortion
Recurrent miscarriage is 3 or more consecutive,
spontaneous pregnancy losses, before viability in the
same pattern.
Septic abortion Most often associated with criminal
induced abortion. Metritis is usual outcome, but
parametritis, peritonitis, endocarditis, and septicemia
may all occur
Therapeutic abortion Done if continuation of pregnancy may
threaten the life of women or seriously impair her health e.g
heart disease , advanced hypertensive vascular disease ,
invasive carcinoma of the cervix, or in case of severe congenital
abnormality of fetus which is incompatible with life.
Factors to betaken into account when discussing these options with patients
1. Type of miscarriage.
2. Gestation at which miscarriage is diagnosed those dx At 11 weeks and above where
there is a missed miscarriage and an embryo measuring significantly less than
expected, these patients are at risk of heavier bleeding compared with earlier
gestations and should be warned of such. Surgical evacuation may be preferable as
the first line of treatment. If the preference is for medical evacuation, then this may
be more appropriately carried out in an inpatient setting.
3. Facilities available at individual units : easy and rapid access to emergency unit.
4. Medical history, for example cardiac disease and sickle cell anaemia.
5. Patient choice.
6. Cost
18.
Expectant management
• Upto 85% of miscarriages will resolve spontaneously within 3 weeks of the diagnosis.
• The rate of success in part depends on the length of delay in intervention.
• The recent NICE guidance advocates that all women should be offered expectant
management as first line unless there are extenuating circumstances.
• A repeat TVS should be offered at 2wks to ensure complete miscarriage—can be repeated
after another 2wks if a woman wishes to continue with conservative management.
• Patients should be offered surgical evacuation at a later date if expectant management is
unsuccessful
↓
-
TransVaginal US
To give Anti-Dprophylaxis
Anti-D should be given to all non-sensitized Rh-
ve patients in the following circumstances:
1. <12wks (250 IU IM):
*uterine evacuation (medical and surgical)
*ectopic pregnancies.
2. >12wks: all women with bleeding (250 U IM
before 20wks and 500IU IM after 20wks)
&
&
L
-
21.
Medical management
• Prostaglandinanalogues (usually misoprostol) are used, administered
orally or vaginally, usually with antiprogesterone priming (mifepristone)
24–48h prior.
• Oxytocin:
Successful induction of 2nd trimester abortion is possible with high doses of oxytocin administered in
small volumes of IV fluids.
Bleeding may continue for up to 3wks after medical uterine evacuation, but completion rates up to 80–
90% can be expected under 9wks gestation.
22.
Women should bewarned that passage of
pregnancy tissue may be associated with pain
and heavy bleeding (though unusual for the
majority) and 24h telephone advice and facilities
for emergency admission should be available
23.
Surgical management
An ERPCshould be performed in patients
who have excessive or persistent bleeding
or request surgical management.
Abdominal Hysterotomy :
Failure or contraindication for medical
induction during the late 2nd trimester
Suction curettage,dilatation and
curettage should be used.
Complications of surgicalmanagement
1. Infection.
2. Haemorrhage.
3. Uterine perforation (and rarely intraperitoneal injury).
4. Retained products of conception.
5. Intrauterine adhesions.
6. Cervical tears.
7. Intra-abdominal trauma.
Uterine and cervical trauma may be minimized by administering
prostaglandin (misoprostol or gemeprost) before the procedure.
9
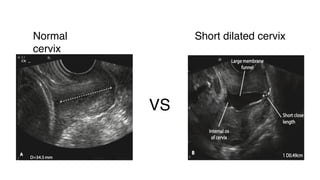
Cervical insufficiency
Painless dilatationof cervix in the 2ndor early in the 3rd trimester
Diagnosis
History 2ndor early in the 3rd trimester loss
Ultrasound +- TVS
↳ 9



![First‐trimester miscarriage
• It is thought that up to 95% of chromosomally abnormal embryos
result in miscarriage
• Trisomies: 68%, mainly trisomy 16, 21 and 22.
• Triploidy: 17.1%.
• Monosomy: 9.8% (XO Turner’s syndrome).
Other causes implicated in first‐trimester miscarriage include the
following.
• Maternal disease: antiphospholipid syndrome, diabetes,thyroid disease.
• Drugs: methotrexate, some antiepileptic drugs.
• Uterine abnormalities: the role of fibroids is uncertain but they may be implicated [5].
• Infection: varicella, rubella and other viral illnesses
&](https://image.slidesharecdn.com/bleedinginearlypregnancy-250906191551-08add4e8/85/bleeding-in-early-pregnancy-during-pregnancy-pdf-6-320.jpg)