
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Embryology of GIT malformations by Dr. Yeneneh
Similar to Embryology of GIT malformations by Dr. Yeneneh (20)
Recently uploaded
Recently uploaded (20)
Embryology of GIT malformations by Dr. Yeneneh
- 1. Embryogenesis of GI Tract and it’s Developmental Anomalies Moderator: Dr. Maru (Consultant Pediatric Surgeon) Presenter: Yeneneh Yirga(GSR-I)
- 2. Outline Introduction Foregut Development and Anomalies Midgut Development and Anomalies Hindgut Development and Anomalies
- 3. Introduction • Congenital GI malformations are spectrum of diseases that occur 2ry to anomalies in the GI tract during the intrauterine life • Overall prevalence 7.28 per 10,000 live births • Congenital absence, atresia, and stenosis of the small intestine (2.37/10,000) • Tracheoesophageal fistula (2.06/10,000) • Account for ~1% neonatal deaths worldwide • 14.8% of all congenital anomalies (T. Tessema , 1995, Gondor) • Causes of Neonatal Intestinal obstruction: ARM (57%)>> intestinal atresia >> Hirschsprung’s disease (Amezene T, TASH, 2017)
- 4. Cont’d • Neonatal Gastrointestinal surgical emergencies (Endale Tefera, TASH, 2007): • ARM ~45% • Intestinal atresia & EA/TEF ~20% • Associated with increased mortality; • Only 1 out of 12 EA/TEF discharged alive • 7 out of 12 Jejunal atresias died
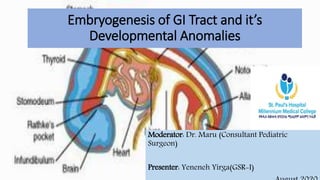
- 5. Embryologic Development of GIT cephalocaudal and lateral folding, form the primitive gut aka Primordial gut, which start at 4th weeks of GA. In the cephalic and caudal parts of the embryo, the primitive gut forms a blind ending tube, the foregut and hindgut, respectively. Cranial end > Oropharyngeal Membrane Caudal end > Cloacal Membrame The middle part, the Midgut, remains temporarily connected to the yolk sac by means of the vitelline duct, or yolk stalk.
- 7. Cont’d
- 8. Molecular Regulation of Gut Tube Development Development can be influenced by a variety of processes, including genetic endowment; the biologic clock; cellular, neural, and hormonal regulatory mechanisms; and the environment Specification is initiated by a concentration gradient o f retinoic acid (RA). • Pharynx =little or no • Colon =the highest concentration. Based on this gradient different transcription factors will be expressed in different regions o f the gut tube. • SOX 2: esophagus and stomach; • PDXl :the duodenum; • CDXQ:the small intestine • CDXA:the large intestine and rectum Epithelial -Mesenchymal interaction is initiated by SONIC HEDGEHOG (SHH) expression throughout the gut tube & expression o f the HOX genes in the mesoderm. As a general rule, maturation tends to occur along craniocaudal and proximodistal axes.
- 9. Cont’d Other important components In the development of the GI tract: Left right Assymetry Digestion and Absorption Vascularization Neural and Motor function Hormonal Regulation Host defence
- 10. Cont’d Postconceptional age 20 weeks 25 weeks 30 weeks 35 weeks 40 weeks Mouth Salivary glands Swallow reflex present Lingual lipase Sucking reflex present Esophagus Muscle layers present Striated epithelium present Poor lower esophageal sphincter tone Stomach Gastric glands present G cells appear Gastric secretions present Slow gastric emptying * Pancreas Exocrine and endocrine tissue differentiate Zymogen present Reduced trypsin, lipase * Liver Lobules form Bile secreted Fatty acids absorbed * Intestine Crypts and villi form Glucose transport present Dipeptidese, sucrase, and maltase active Lactase active Colon Crypts and villi recede Meconium passed • Anatomic and functional maturation of the gastrointestinal tract
- 11. Mesenteries and peritoneum Portions of the gut tube and its derivatives are suspended from the dorsal and ventral body wall by mesenteries. Intraperitoneal vs retroperitoneal organs Peritoneal ligaments are double layers of peritoneum (mesenteries) that pass from one organ to another or from an organ to the body wall. Dorsal mesentery extends from the lower end of the esophagus to the cloacal region of the hindgut, at 5th week. Ventral mesentery : terminal part of the esophagus, the stomach, and the upper part of the duodenum derived from the septum transversum Growth of the liver into the mesenchyme of the septum transversum divides the ventral mesentery into the lesser omentum and falciform ligament
- 12. Foregut Esophagus At around 4 weeks the respiratory diverticulum (lung bud) appears at the ventral wall of the foregut. The tracheoesophageal septum gradually partitions this diverticulum. The foregut divides into a ventral portion, the respiratory primordium and a dorsal portion, the esophagus. At first, the esophagus is short but with descent of the heart and lungs, it lengthens rapidly. striated muscle vs smooth muscle
- 13. EA/TEF • Unknown cause; Incomplete fusion of the folds results in a defective tracheoesophageal septum and abnormal connection. • M:F = 1.26 : 1 • 1 in 2500 to 3000 live births • Associated congenital malformation : 50% - 70% • Gross classification A-E • EA with distal TEF ~ 85% (Type C)
- 14. Cont’d • Not commonly diagnosed prenatally • Prenatal: polyhydraminos & absent/small stomach bubble • Postnatal • Vomiting, frequent regurgitation, aspiration • NG tube & x-ray
- 15. Cont’d Congenital Esophageal Stenosis : • 1 in 25,000 - 50,000 births • usually in the lower 1/3 • 17 - 33% associated with other malformations Classifications: 1. membranous web or diaphragm 2. fibromuscular thickening 3. stricture secondary to tracheobronchial remnants • c/m: progressive dysphagia and vomiting Congenital Diaphragmatic Hernia : • 2ry short esophagus
- 16. Stomach • fusiform dilation of the foregut at 4th wks. • different rates of growth in various regions of its wall and the changes in position of surrounding organs • stomach rotates 90° clockwise around its longitudinal axis. • Vagus N. >> LARP • formation of greater and lesser curvatures • Caudal/pyloric moves to right & upward • Cephallic/cardiac moves to left & slightly downward
- 17. Cont’d • Rotation about the longitudinal axis pulls the dorsal mesogastrium create omental bursa (lesser peritoneal sac) • spleen primordial appears as a mesodermal proliferation between the two leaves of the dorsal mesogastrium Lienorenal ligament gastrolienal ligament • Dorsal mesogastrium > Greater Omentum • Ventral mesogastrium > lesser omentum & falciform ligament • Ligamentum teres hepatis • Hapatoduodenal ligament • Epiploic foramen of Winslow
- 18. Duodenum • terminal part of the foregut and the cephalic part of the midgut at 4th wk Junction: just distal to liver bed • Stomach rotation > C-shaped loop • Rapid growth of head of pancreases > right side position • At 6th wk, the lumen is obliterated by proliferation of cells in its walls & recanalized shortly thereafter.
- 19. Duodenal Atresia and Stenosis • most common sites of neonatal intestinal obstruction • Atresia >> stenosis • 1 in 5 - 10,000 live births : M >> F • 50% have associated congenital anomalies • Intrinsic –Vs- Extrinsic lesion • Gray and Skandalakis Classification • Type 1 (92%): There is an obstructing septum (web) formed from mucosa and submucosa with no defect in the muscularis. The mesentery is intact. • Type 2 (1%): A short fibrous cord connects the two blind ends of the duodenum. The mesentery is intact. • Type 3 (7%): There is no connection between the two blind ends of the duodenum. There is a V-shaped mesenteric defect.
- 20. Cont’d
- 21. Liver , Gall Bladder & Pancreas • Liver • Primordium appears in the middle of the 3rd week. • Penetrate the septum transversum. • Gallbladder and the cystic duct. • Ventral outgrowth from the bile duct. • Pancreas • Dorsal and ventral buds. • Rotation of duodenum fuses the parts.
- 22. Midgut • Formation of Primary intestinal loop, the apex being vitelline duct. Physiological umbilical hernia at 6th week Rotation of the midgut: total of 270° CCW direction along SMA. • 90° during herniation • 180° during return of intestinal loops into the abdominal cavity Retraction of herniated loops at 10th-12th wk • Cecal Bud swelling: at 6th wk, as elevation on antimesenteric border
- 23. Cont’d Fixation & Mesenteries of intestinal loops Abnormalities in the mesentery • Mobile Cecum : 2ry persistence of portion of mesocolon. • In extreme cases >> cecal or colonic volvulus. • Retrocolic pockets 2ry incomlete fusion • Retrocolic hernia
- 24. Gut Rotation Defects/ Midgut Malrotations Nonrotation: occurs when the intestine does not rotate as it reenters the abdomen • caudal limb of the midgut loop returns to the abdomen first • Duodenojejunal limb on the right side of the abdomen and Cecocolic limb on the left • Midgut volvulus due to narrow mesenteric pedicle Reversed Rotation : the midgut loop rotates in a clockwise direction • duodenum lies anterior to SMA • transverse colon lies posteriorly
- 25. Cont’d Incomplte rotation: arrested CCW rotation at/near 180° • cecum lies just inferior to the pylorus, in subhepatic/ RUQ position • cecum is fixed to the posterolateral abdominal wall by peritoneal bands • Midgut volvulus occur 2ry the obstructing band & abnormal fixation • peritoneal bands and volvulus of the intestine cause intestinal atresia (duodenal obstruction)
- 26. Jejunoileal Atresias and Stenoses • 1 in 5000 of live births , M=F • Common in LBW & premature infants • 2ry intrauterine vascular ‘accidents’, affecting single or multiple segments of the already developed intestine, or • 2ry problems of gut differentiation: HOX genes • maternal vasoconstrictive medications, maternal cigarette smoking during 1st TMPx increase the risk of atresia • Rarely associated extra intestinal anomalies (<10%), since occurrence is relatively late • Atresias ~ 95%, Stenosis ~ 5%
- 27. Cont’d Grosfeld classification system Type I: webs(luminal diaphragm) Mucosal atresia with intact bowel and mesenetery Type II: Blind ends separated by a fibrous cord Type III(a): Blind ends separated by a V-shape mesenteric defect Commonest ~50 % Type III(b): Apple-peel atresia Type IV: Multiple atresias (string of sausages) : 20-35%
- 28. Colonic Atresia • Rare cause of neonatal GI obstruction • 2-15 % of intestinal atresias • ~1 in 20,000 live births • 1/3 associated with other congenital malformations • Type I : mucosal atresia • Type II: atretic ends are separated by fibrous cord • Type III: atretic ends separated by V-shaped mesenteric gap • C/M: abdominal distention, bilious emesis, and failure to pass meconium.
- 29. GIT Duplications • Rare, 1 in 4500 live births • 2 types : cystic >> tubular • Proposed etiologic factors: persistent embryonic diverticulum defect in the recanalization partial twinning theory ‘split notochord’ theory • jejunum/ileum(50%)>>esophagus(20%) >other • heterotopic mucosa in 25–30% • Located on mesenteric side
- 30. Vitelline Duct Abnormalities Meckel diverticulum • relatively common • 3-6 cm long, is a true diverticula • On antimesentric border of ileum • Majorty of cases are asymptomatic • May contain hetrotropic pancreatic tissue or gastric mucosa • Rule of Two Other abnormalities : fibrous cord, fistulas, Omphaloenteric cysts
- 31. Body wall Defects OMPHALOCELE • 1 to 2.5 per 5000 live birth • M>>F • 2ry failure of the body folds to complete their journey -Vs- failure of retraction of herniated bowel loops • Bowel +/- solid organs in omphalocele sac through the umbilicus • Ass. Other congenital malformations (~45% cardiac anomalies) • High mortality (~25%) • Dx : Prenatal sonography • Surgical mgt not urgent, unless raptured
- 32. GASTROSCIASIS • Commonest; 2 to 4.9 per 10,000 live birth • Maternal age <21 yrs • 2ry failure of migration of the lateral folds • Usually on right side • Freely floating bowel • Other congenital anomalies <10 % • Concomitant bowel atresia (7-28%) • Dx: prenatal sonography • Needs urgent surgical intervention Umbilical Cord Hernias: bowel loops later herniate again through an imperfectly closed umbilicus • Rare phenomenon
- 33. Hind Gut • Cloaca is an endoderm lined chamber that is in contact with the surface ectoderm at the cloacal membrane. • At 7th week cloaca is divided into dorsal and ventral parts by a wedge of mesenchyme, the urorectal septum, creating; • rectum and cranial part of the anal canal dorsally & • urogenital sinus ventrally • In b/n, the tip of the urorectal septum forms the perineal body • Ectoderm in the region of the proctodeum on the surface of part of the cloaca proliferates and invaginates to create the anal pit
- 34. Anal Canal • Superior 2/3 derived from hindgut • Inferior 1/3 develops from the anal pit • junction of the epithelium roughly indicated by the irregular pectinate line • ~2 cm superior to the anus is the anocutaneous line (white line) • Keratinized epithelium of the anus is continuous with that of surrounding skin • The other layers of the wall of the anal canal are derived from splanchnic mesenchyme.
- 35. ARMs (Anorectal Malformations) • ~1 in 4-5,000 : M > F • Risk of ARM in the second child is ~1% • Arrest of the caudal descent of the urorectal septum to the cloacal membrane. • ARMs with out fistulas are rare • Can be low, intermediate or high • Associated anomalies (50-60 %): Sacral deformities (commonest), Spinal problems (e.g. Tethered cord), Genitourinary defects • Generally high deformities are associated with poor bowel function,fistula tracts, difficult surgical repairs (requiring multiple procedures), more malformations and poor prognosis.
- 36. Classification of infants with ARMs MALES • Rectoperineal fistula • Rectourethral bulbar fistula • Rectourethral prostatic fistula • Rectobladderneck fistula • Imperforate anus without fistula • Rectal atresia/rectal stenosis FEMALES • Rectoperineal fistula • Rectovestibular fistula • Persistent Cloaca • Complex malformations • Imperforate anus without fistula • Rectal atresia/rectal stenosis
- 37. Hirschsprung Disease/ congenital megacolon • absence of ganglion cells in the myenteric and submucosal plexuses of the distal intestine • 1 : 5,000 live births • ‘transition zone’ located at; • rectum or rectosigmoid colon (~80%) • proximal colonic involvemen (~10%) • total colonic aganglionosis +/- distal small intestine (5-10%) • Short Vs Long Segment • Presentation is variable : • Neonatal bowel obstruction (50-90%) • Chronic constipation • Enterocolitis (10%)
Editor's Notes
- A study done in India shows : The predominant system involved was Musculoskeletal system (33.2%) followed by gastro-intestinal (GI) system (15%).
- Mortality depends on: Associated congenital malformations, Early –vs- delayed Dx & presentation, timely intervention & perioperative care.
- Development o f the primitive gut and its derivatives is usually discussed in four sections: The pharyngeal gut, or pharynx :extends from the oropharyngeal membrane to the respiratory diverticulum. The foregut lies caudal to the pharyngeal tube and extends as far caudally as the liver outgrowth. The Midgut begins caudal to the liver bud and extends to the junction of the right two-thirds and left third of the transverse colon in the adult. The hindgut extends from the left third of the transverse colon to the cloacal membrane.
- 1. The asymmetry of the contents of the abdomen is more obvious than in any other part of the body. Only in congenital disorders of the heart are the clinical consequences of deranged asymmetry greater than in the GI tract. Examples of disorders that may be caused by disturbances of lateral development include: ● Situs inversus abdominus ● Polysplenia or asplenia ● Pancreas divisum or annular pancreas ● Malrotation 2. The arterial bed develops as three ventral out buddings from the aorta to form the celiac axis, and the superior and inferior mesenteric arteries. Mesenteric blood flow is regulated at two points (the arteriole and the precapillary sphincter) and controlled at two levels (intrinsic and extrinsic). Intrinsic control by local factors regulates blood flow in response to changes in arterial pressure and tissue oxygenation, such as those caused by vascular constriction or feeding. Extrinsic regulation is mediated by sympathetic input from the splanchnic nerves. 3. The neural crest cells and muscle cells differentiate to form the three layers of muscle that surround the mucosa and the neural network that regulates its function. Control of motor function is provided primarily by the enteric nervous system (a subsystem of the autonomic nervous system), which is composed of a variety of plexuses of nerve cell bodies and interneuronal circuits. 4. Glucocorticoids and thyroid hormone interact with cellular signals in the maturation of the intestinal epithelium. Numerous regulatory gut peptides are also produced in the developing GI tract. Some of these peptides function as true hormones (eg, gastrin, cholecystokinin, motilin, pancreatic polypeptide, and somatostatin), whereas others have paracrine or neurocrine function (eg, gastric inhibitory peptide, bombesin, vasoactive intestinal polypeptide, neurotensin, enteroglucagon, and peptide YY). 5. T cells and B cells are produced as early as 14 weeks gestation. However, antigenic stimulation of the lamina propria cells does not occur until after birth. Secretory immunoglobulin A (IgA) is present in very low concentrations in fetal life, as the newborn intestine has few IgA-producing plasma cells. Therefore, preterm infants are unable to form antibodies to exogenous protein.
- * Full maturation occurs postnatally.
- The striated muscle of the superior third of the esophagus is derived from mesenchyme in the 4th and 6th pharyngeal arches. The smooth muscle, mainly in the inferior third of the esophagus, develops from the surrounding splanchnic mesenchyme.
- ** Environmental factors that have been implicated include the use of methimazole in early pregnancy, prolonged use of contraceptive pills, progesterone and estrogen exposure, maternal diabetes, and thalidomide exposure. EA is occasionally seen in the fetal alcohol syndrome and in maternal phenylketonuria. ** Chromosomal anomalies are found in 6–10%. The total number of trisomy 18 cases exceeds the total number of trisomy 21 cases. ** The anomalies are most common in cases of EA without TEF and are least common in cases of H-type TEF. Complex cardiac deformities may account for most of the deaths associated with EA malformation.
- ** Stenosis may be caused by incomplete recanalization , vascular abnormalities , or accidents that compromise blood flow.
- Congenital anomalies of stomach are uncommon, but includes: iHPS Microgastria Gastric Atresia Antral Mucosal Diaphragm Duplication Cyst Malrotation
- ** The terminal part o f the foregut and the cephalic part o f the midgut form the duodenum.
- ** This intrinsic lesion is most commonly believed to be caused by a failure of recanalization of the fetal duodenum resulting in complete obstruction. Early in the fourth week of gestation, the duodenum begins to develop from the distal foregut and the proximal midgut. During the fifth and sixth weeks of gestation, the duodenal lumen temporarily obliterates due to proliferation of its epithelial cells. Vacuolation due to degeneration of the epithelial cells during the 11th week of gestation then leads to duodenal recanalization. An embryologic insult during this period can lead to an intrinsic web, atresia, or stenosis. ** The extrinsic form of duodenal obstruction is due to defects in the development of neighboring structures such as the pancreas, a preduodenal portal vein, or malrotation and Ladd’s bands. ** Most stenoses involve the horizontal (third) and/or ascending (fourth) parts of the duodenum. Because of the stenosis, the stomach’s contents (usually containing bile) are often vomited.
- ** is characterized by rapid elongation of the gut and its mesentery, resulting in formation of the primary intestinal loop. ** During the 10th week, herniated intestinal loops begin to return to the abdominal cavity. Although the factors responsible for this return are not precisely known, it is thought that regression o f the mesonephric kidney, reduced growth of the liver, and expansion of the abdominal cavity play important roles. ** Jejunum and ileum retain their mesenteries w/c is fan-shaped mesentery that passes from the duodenojejunal junction inferolaterally to the ileocecal junction. ** The primordium of the cecum and appendix, the cecal swelling, appears in the sixth week as an elevation on the antimesenteric border of the caudal limb of the midgut loop.
- N.B: Malrotation is an integral part of congenital diaphragmatic hernia and all abdominal wall defects. Associated anomalies are found in 30% to 60% of patients with malrotation. **reverse rotation : the small intestine lies on the left side of the abdomen and the large intestine lies on the right side, with the cecum in the center. The transverse colon eventually lies behind the vessels, which may result in acute or chronic colonic obstruction.
- ** commonest intestinal atresia is duodenal atresia. ** Intrauterine vascular disruption can lead to ischemic necrosis of the bowel with subsequent resorption of the affected segment/s. Vascular accidents occur 2ry malrotations, volvulus, abdominal wall defects, intussusception, thromboembolic occlusions, transmesenteric internal hernias, …. ** Presenting features include maternal polyhydramnios (jejunal>>ileal), bilious emesis, abdominal distention, jaundice, and failure to pass meconium on the first day of life.
- ** The Grosfeld classification system separates these defects into four groups, with an additional consideration for type III(b). This classification has significant prognostic and therapeutic value as it emphasizes the importance of associated loss of intestinal length, abnormal collateral intestinal blood supply, and concomitant atresia or stenosis. Regarding classification, the most proximal atresia determines whether the atresia is classified as jejunal or ileal atresia. Multiple atresias are found in up to 30% of patients. ** As with stenosis, there is no foreshortening of the bowel in type I atresias.Type II also have relatively normal bowel length ** Type III(b) atresia (apple-peel, Christmas tree, or Maypole deformity) consists of a proximal jejunal atresia, absence of the superior mesenteric artery beyond the origin of the middle colic branch, agenesis of the dorsal mesentery, a significant loss of intestinal length, and a large mesenteric defect. ** Intestinal stenosis is more likely to create diagnostic difficulty when compared to intestinal atresia. Intermittent partial obstruction or malabsorption may improve without treatment. Clinical investigations can initially be normal. However, these babies usually develop failure to thrive and ultimately progress to complete intestinal obstruction and require exploration.
- Type I consists of mucosal atresia with an intact bowel wall and mesentery. In type II, the atretic ends are separated by a fibrous cord. In type III, the atretic ends are separated by a V-shaped mesenteric gap. Type III lesions are the most commonly occurring lesions overall, while types I and II are seen more commonly distal to the splenic flexure.
- ** Alimentary tract duplications present with a wide range of symptoms including abdominal distension and/or pain, obstruction, bleeding, respiratory compromise, or a painless mass. Generally, the symptoms are related to size, location, type of duplication, and presence of heterotopic mucosa. Most (80%) present before 2 years of age; prenatal ultrasound is detecting duplications as early as 16 weeks. The majority of duplications are cystic and the remaining are tubular. ** Gastric tissue is the most common type of ectopic mucosa encountered followed by both exocrine and endocrine pancreatic tissue. Ectopic gastric mucosa may lead to peptic ulceration with subsequent hemorrhage or perforation.
- Rule of two: Prevalence ~2% Size/length ~2 inches (3-6 cms) Site ~2 feets (40-60cms) from ileocecal valve Symptomatic in ~2% of cases Sxs occur after the age of 2 yrs M:F = 2:1 2 ectopic tissue; gastric followed by pancreatic tissue
- ** Up to 45% of patients with omphalocele have been reported to have a cardiac abnormality including ventricular septal defect, atrial septal defect, ectopia cordis, tricuspid atresia, coarctation of the aorta, and persistent pulmonary hypertension of the newborn. Chromosomal abnormalities can be found in up to 20%, and an association with Down syndrome has also been reported. ** Ompalocele sac consists covering layers of the umbilical cord and includes amnion, Wharton’s jelly, and peritoneum.
- ** The etiology for gastroschisis is less clear. One theory suggests that gastroschisis results from failure of the mesoderm to form in the anterior abdominal wall. Currently, the ventral body folds theory, which suggests failure of migration of the lateral folds (more frequent on the right side), is most widely accepted. This implies a gastroschisis develops early in gestation and prior to development of an omphalocele. Due to the increasing incidence of gastroschisis, there are a number of possible causative factors including tobacco, certain environmental exposures, lower maternal age and low socioeconomic status, all suggested by epidemiologic studies, but not proven.
- ** The hindgut gives rise to the distal third of the transverse colon, the descending colon, the sigmoid, the rectum, and the upper part of the anal canal. The endoderm of the hindgut also forms the internal lining o f the bladder and urethra. ** In early embryos, the cloaca is a chamber into which the hindgut and allantois empty. The expanded terminal part of the hindgut, the cloaca, is an endoderm-lined chamber that is in contact with the surface ectoderm at the cloacal membrane. ** The upper part (two-thirds) of the anal canal is derived from endoderm o f the hindgut; the lower part (one-third) is derived from ectoderm around the proctodeum. ** Subsequent degeneration of the cloacal membrane (now called the anal membrane) establishes continuity between the upper and lower parts of the anal canal. ** The cloaca plays a crucial role in anorectal development. New information indicates that the urorectal septum does not fuse with the cloacal membrane; therefore, an anal membrane does not exist. After the cloacal membrane ruptures by apoptosis (programmed cell death), the anorectal lumen is temporarily closed by an epithelial plug(which may have been misinterpreted as the anal membrane). Mesenchymal proliferations produce elevations of the surface ectoderm around the epithelial anal plug. Recanalization of the anorectal canal occurs by apoptotic cell death of the epithelial anal plug, which forms the anal pit (proctodeum).
- ** Approximately 2 cm superior to the anus is the anocutaneous line(white line). This is approximately where the composition of the anal epithelium changes from columnar to stratified squamous cells. At the anus, the epithelium is keratinized (made keratinous) and continuous with the skin around the anus. ** Because of its hindgut origin, the superior two thirds of the anal canal are mainly supplied by the superior rectal artery, the continuation of the inferior mesenteric artery (hindgut artery). The venous drainage of this superior part is mainly via the superior rectal vein, a tributary of the inferior mesenteric vein. The lymphatic drainage of the superior part is eventually to the inferior mesenteric lymph nodes. Its nerves are from the autonomic nervous system. ** Because of its origin from the anal pit, the inferior one third of the anal canal is supplied mainly by the inferior rectal arteries, branches of the internal pudendal artery. The venous drainage is through the inferior rectal vein, a tributary of the internal pudendal vein that drains into the internal iliac vein. The lymphatic drainage of the inferior part of the anal canal is to the superficial inguinal lymph nodes. Its nerve supply is from the inferior rectal nerve; hence, it is sensitive to pain, temperature, touch, and pressure. ** The differences in blood supply, nerve supply, and venous and lymphatic drainage of the anal canal are important clinically, as when one may be considering the metastasis(spread) of cancer cells. The characteristics of a carcinoma (cancer arising in the epithelial tissue) in the two parts is also different. Tumors in the superior part are painless and arise from columnar epithelium, whereas tumors in the inferior part are painful and arise from stratified squamous epithelium.
- ** Lower urethral fistulas are usually associated with good-quality muscles, a well-developed sacrum, a prominent midline groove, and a prominent anal dimple. Higher urethral fistulas are more frequently associated with poor-quality muscles, an abnormally developed sacrum, a flat perineum, a poor midline groove, and a barely visible anal dimple. ** Lumbosacral anomalies such as hemivertebrae, scoliosis, butterfly vertebrae, and hemisacrum are common. The most frequent spinal problem is tethered cord. ** The evaluation in every child with imperforate anus must include an ultrasound (US) of the kidneys and abdomen to evaluate for the presence of hydronephrosis or any other urologic obstructive process.
- ** By 13 weeks the neural crest cells have undergone a process of migration through the gastrointestinal tract from proximal to distal, after which they differentiate into mature ganglion cells. ** There are two main theories why this process is disturbed in children with HD. The first possibility is that the neural crest cells never reach the distal intestine due to early maturation or differentiation into ganglion cells. The second possibility is that the neural crest cells reach their destination, but fail to survive or differentiate into ganglion cells due to an inhospitable microenvironment. ** Approximately 80% of children have a ‘transition zone’ in the rectum or rectosigmoid colon. Another 10% have more proximal colonic involvement, and about 5–10% have total colonic aganglionosis with variable involvement of the distal small intestine. Rarely, babies are afflicted with near-total intestinal aganglionosis. ** Approximately 50% to 90% of children with HD present during the neonatal period with abdominal distension, bilious vomiting, and feeding intolerance suggestive of distal intestinal obstruction. Delayed passage of meconium beyond the first 24 hours is characteristic but is only present in approximately 90% of children with HD. In some patients cecal or appendiceal perforation may be the initial event. ** Approximately 10% of children with HD present with fever, abdominal distention, and diarrhea due to Hirschsprung associated enterocolitis (HAEC), which may be chronic, or may be severe and life-threatening. Because Hirschsprung disease is generally thought of as causing constipation, presentation with diarrhea may be confusing and the diagnosis may not be considered. ** Plain & contrast Radiographs, anorectal manometry, Rectal Bx (definitive Dx) are important in evaluation of HD.