Download as PDF, PPTX
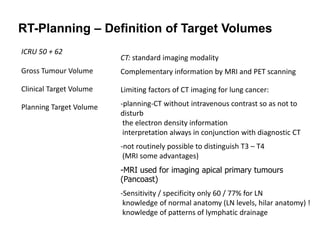
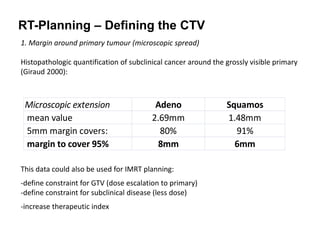
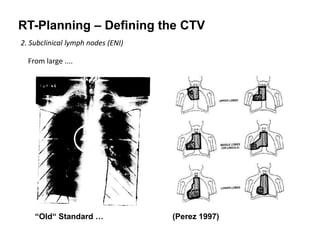
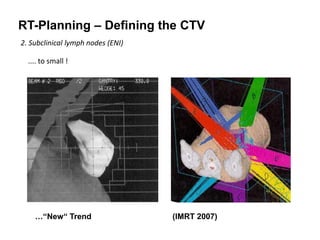
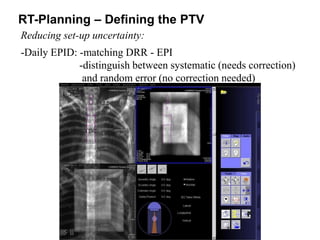
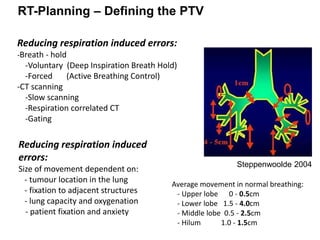
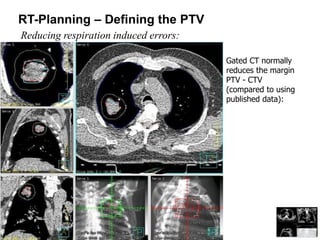
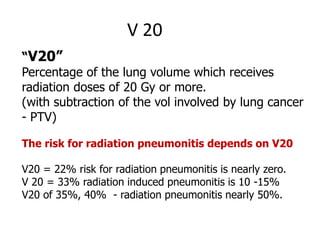
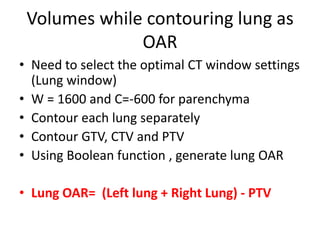



This document summarizes guidelines for radiotherapy planning for lung cancer. It discusses: - Defining the gross tumor volume (GTV) based on imaging like PET which can help reduce margins. - Adding margins to the GTV to create the clinical target volume (CTV) accounting for microscopic spread. There is debate around elective nodal irradiation. - Further expanding the CTV to create the planning target volume (PTV) accounting for set-up uncertainty and tumor motion. Techniques like gating can help reduce this. - Contouring the lungs as organs at risk and calculating dosimetric parameters like V20 and V5 to quantify lung dose and risk of toxicity. Dose needs to


















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




