Downloaded 31 times
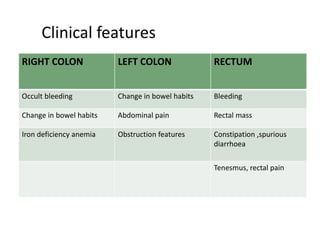
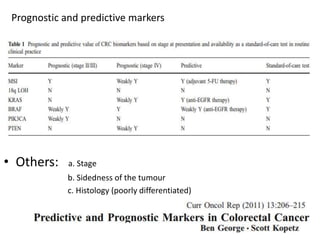
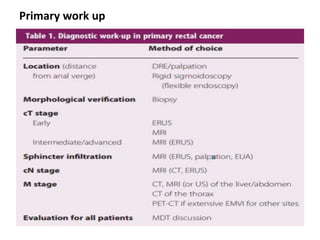
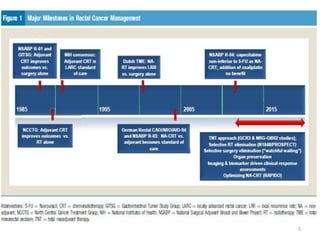
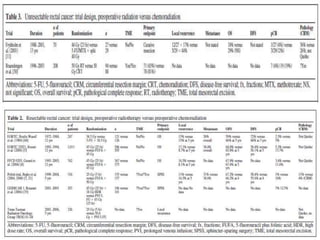
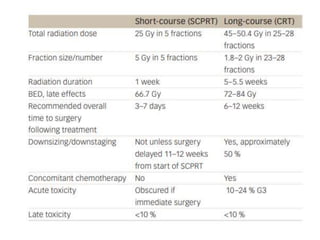



This document discusses updates in radiation therapy for colorectal cancers. It covers clinical features and prognostic markers for different locations of colorectal cancer. It discusses the goals and need for a multidisciplinary approach in treating rectal cancers. It compares pre-operative vs postoperative chemoradiation and short course vs long course radiation. It also discusses omitting adjuvant chemotherapy for some patients and contouring guidelines for radiotherapy planning.









































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













