Downloaded 69 times
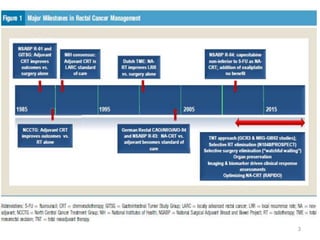
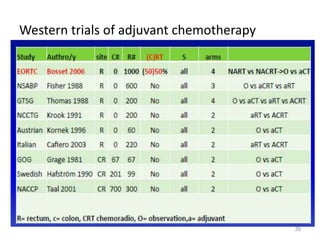
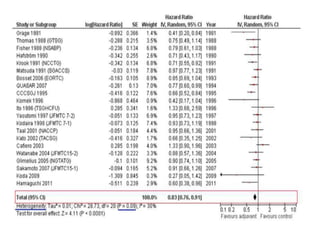
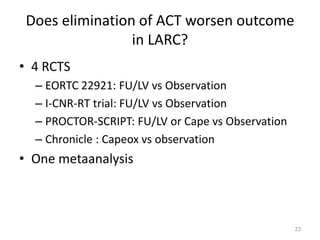
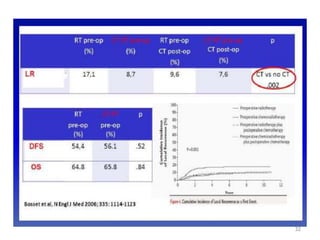
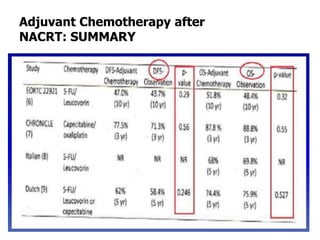
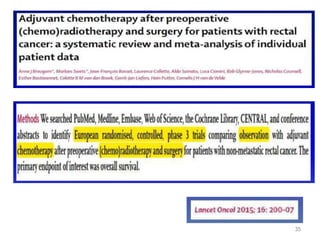

1) Adjuvant chemoradiation improves local control for locally advanced rectal cancer compared to surgery alone based on multiple trials from the 1980s and 1990s. 2) Recent European trials have found no clear benefit of adjuvant chemotherapy after neoadjuvant chemoradiation and surgery for rectal cancer, with the exception of the QUASAR trial. 3) Adjuvant chemotherapy may be recommended after preoperative chemoradiation for mid-low rectal cancers with lymph node involvement (ypT3N+) or high rectal cancers with stage ypT2-3 based on trial results and expert guidelines.






















































































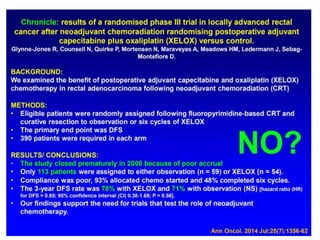
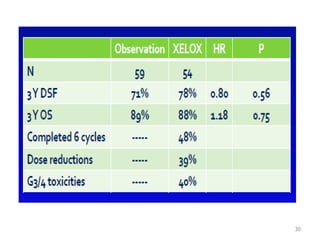
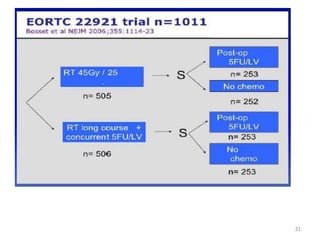
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
