Download as PDF, PPTX
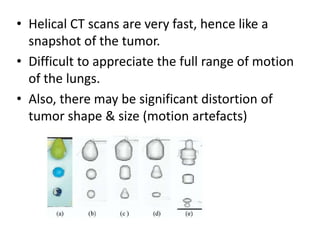



This document discusses motion management techniques for lung cancer radiotherapy. It begins by explaining why motion management is important, as standard CT scans do not fully capture lung tumor motion. It then describes 4DCT and other methods for assessing tumor motion, as well as techniques like ITV, gating, tracking and breath-holding to control for motion. Specific examples of tracking systems like ExacTrac and Cyberknife are provided. Overall, the document provides an overview of the challenges of lung tumor motion and different strategies used to manage it in radiation treatment planning and delivery.








































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)