Downloaded 716 times


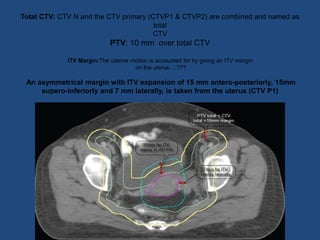


The document provides guidelines for contouring the clinical target volume (CTV) and organs at risk for carcinoma of the cervix treated with 3D conformal radiation therapy or intensity-modulated radiation therapy. The CTV includes the involved lymph nodes (GTV N) and relevant draining nodal groups. The CTV for the primary tumor (CTV-P) includes the gross tumor, uterus, cervix, parametrium, vagina, and ovaries. Detailed guidelines are provided for contouring the lymph node regions, uterus, vagina, and parametrium. A planning target volume (PTV) is created by adding a 10 mm margin to the total CTV. Additional margins are used to create an












































































