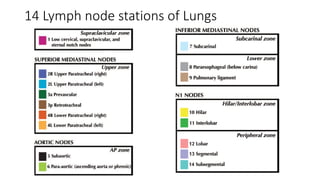
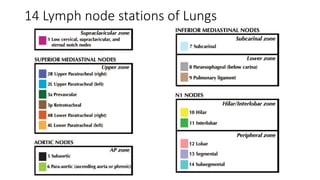


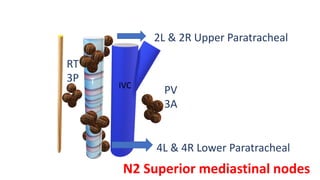
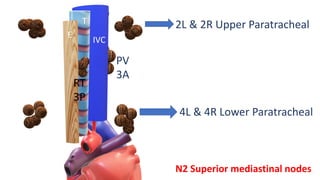
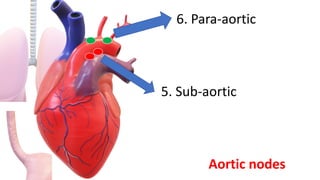
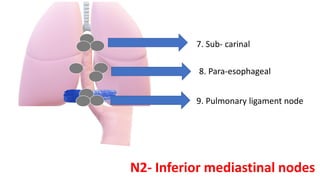
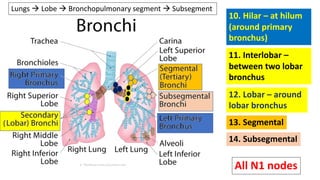
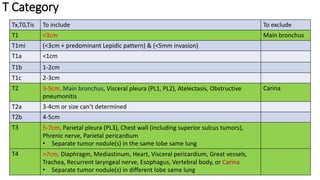
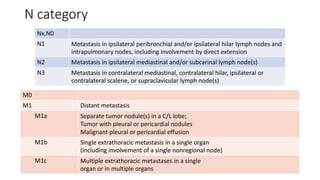
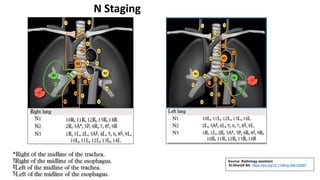
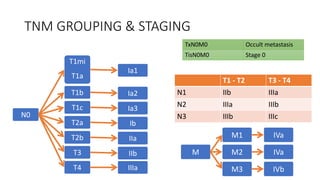

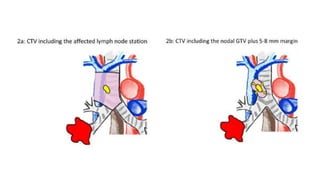
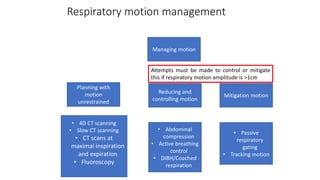
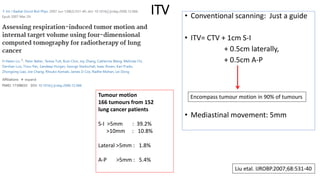

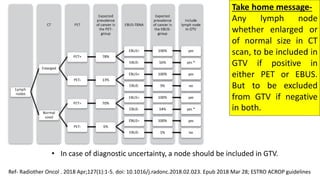


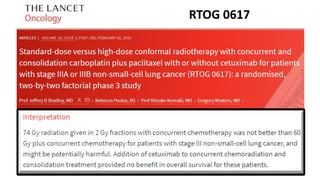
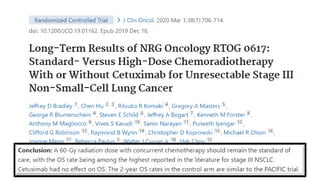
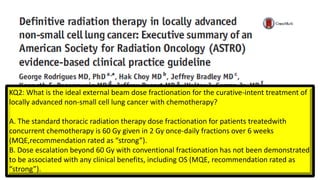

The document outlines radiotherapy techniques and contouring guidelines for treating lung carcinoma, detailing lymph node stations and relevant AJCC classifications for staging. It emphasizes the importance of diagnostic imaging, such as CT and PET scans, for accurate target volume delineation and proposes specific volume margins for treatment planning based on tumor size and location. The document also includes recommendations for dose fractionation in non-small cell lung cancer and adaptive planning strategies to accommodate changes during treatment.











































































